Screening for Cardiovascular Disease with MRI and CAC - Interview with Health Nucleus Part 2
In this post you’ll learn ABOUT:
Health Nucleus tools for assessing cardiovascular disease risk
The role of the Coronary Artery Calcification (CAC) score in assessing risk, particularly for younger people (30s, 40s)
How CAC scores might influence statin use
The limitations of MRI data in assessing risk
How genetic risk factors might influence risk
Combining imaging data, genetic factors and blood tests to further clarify risk
Part 2 - Cardiovascular disease
Be sure to read Part 1!
Longevity Blog (LB):
We’ve talked a little bit about cancer. Another big killer whose risk is a function of how old you are and a number of genetic factors is cardiovascular disease and in particular atherosclerosis.
I understand my risk as a man in his thirties is low for an acute event now, but the disease risk grows with time as the result of a decade on decade buildup of plaque, inflammation and wear and tear on the arteries…
Q: So how does coming to the Health Nucleus help inform someone about how their risk might change as they get older? What could a young person do using this information to minimise their risk of atherosclerosis and cardiovascular disease?

Coronary Artery Calcium Scoring. Credit: Cleveland Clinic
Dr Duchicela: Yeah that’s a great question. So in terms of cardiac assessments, one of the most powerful ones that we do here is the coronary calcium score. This is looking at calcified plaque buildup in the arteries of your heart. Essentially, the more plaque you have the higher your risk is of a heart attack.
You’re right, for someone in their thirties, who’s young, who is otherwise healthy, the chances of you finding plaque are low. Based on the general standard of care in the community, we wouldn’t be getting a coronary calcium score on somebody who’s 35 years old or younger. But here, because we’re under a research protocol, we have a little bit more leeway to push the boundaries in terms of testing in groups that may not otherwise be traditionally tested.
“we’re finding that actually about 15 to 17% of individuals around the age of 40 to 45 or younger actually have significant plaque build up. ”
And so for the coronary calcium score for example we are able to do it on a 35 year old, or 36 year old and we’re finding that actually about 15 to 17% of individuals around the age of 40 to 45 or younger actually have significant plaque build up. So we are probably missing a good amount of people out in the community who have atherosclerosis and calcified plaque in arteries of their heart which will predispose them to heart disease.
So when you come here to Health Nucleus and you if you meet the age requirement of 35 years or older (that’s what do here for the coronary calcium score), you’ll see what your plaque level, your score is, and then we will compare you to other people your same age and gender. So you get a sense of how you stack up to a healthy peer group as well and based on that, we take that into account with your cholesterol numbers and so, let’s say you have high cholesterol numbers, your LDL is elevated and your doctor is trying to push you to be on a statin or a cholesterol medicine.
If you get a coronary calcium score and your score is 0, there’s no calcified plaque seen, then you actually have a pretty good case to make that you shouldn’t be on a statin just yet . A lot of men and women come through here and their doctors are pushing and pushing them to be on a statin because their cholesterol is on the higher side, and we scan them and we get their coronary calcium score and it’s zero or very low that actually is pretty powerful in that it makes it not as urgent to be on a statin and you can talk more about lifestyle modifications and the diet, the exercise and maybe hold off on that statin for awhile longer.
A lot of men and women come through here and their doctors are pushing and pushing them to be on a statin because their cholesterol is on the higher side, and we scan them and we get their coronary calcium score and it’s zero or very low
LB: That’s a really clear answer Keegan, thank you for that.
Q: Could you comment a little bit on what the Health Nucleus can do with the MRI technology in terms of cardiovascular risk?
My heart beating, as observed by the Health Nucleus full body MRI scan and post-processing technology.
Dr Duchicela: For heart attack risk you get most of the assessment from the CT scan and the coronary calcium score. From the MRI what we’re doing is more structure of the heart so this is like what the chambers look like, how large the chambers are, or if they are hypertrophied or thickened because of high blood pressure or if it’s not pumping as well as it should be, like the ejection fraction is low because of early congestive heart failure or some sort of other heart failure. That’s what we get from the MRI. The MRI is more structural. It can find congenital abnormalities of the heart sometimes too, where as the CT scan, the one that involves a little bit of radiation, that is more for heart attack risk.
LB: That’s a good differentiation. Thanks for taking the time to answer that. And so in terms of a young person coming in, you’ve mentioned this kind of threshold of 35 years or older to do the calcium score, I don’t meet that criteria quite yet, but I’ll certainly do it when I get to that point.
Q: What other Health Nucleus tools can sit alongside the diagnostic imaging tests (MRI, CAC score) which can help a young person evaluate their lifetime risk of atherosclerosis?

Dr Duchicela: In terms of genomics, there are some genetic markers that predispose you to very high levels of cholesterol, that would be picked up not only in the blood screen testing, but also in the genetic testing.
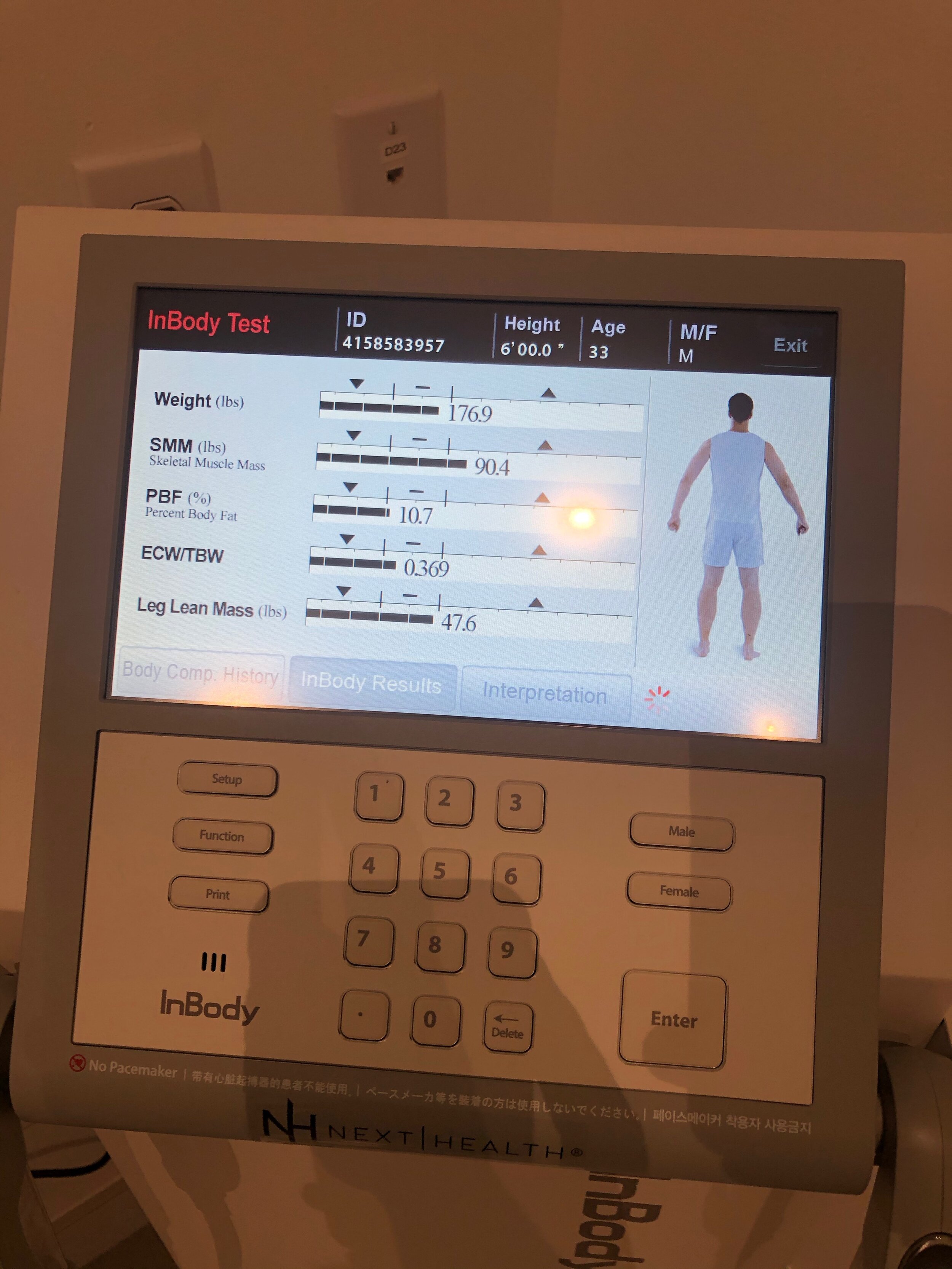
Let's say you're twenty years old and we’re not doing a coronary calcium score, what we would use instead to help predict your overall risk would be the blood test, the lipid panel, your other metabolic markers like your haemoglobin A1c, your fasting sugar. And then from the MRI we’d be looking at your body composition, visceral fat deposition, visceral fat level. With MRI we’re now actually able to quantify pretty accurately your visceral fat volume and compare you to other people your same age and gender.
So those things would build into this risk profile, and then the traditional things like how much you drink, how much you smoke, how much sleep you’re getting, if you have signs of sleep apnoea. Even thirty year olds have sleep apnoea now, so those sorts of things all help build a risk profile for young people if you don’t have let’s say a coronary calcium score.
LB: Right and in terms of the genetic analysis, besides being predisposed to familial hypercholesterolaemia or other acute high LDL cholesterol genetics, Q: Is there another set or group of markers that you might be looking at at an early stage that can show someone’s risk?

Polygenic risk scores from my own Health Nucleus genomic report.
Dr Duchicela: What we currently have is a polygenic risk scale that tells you your relative risk. What we do is we look at gene variants that are more present in groups or individuals that have for example coronary artery disease, or who have had heart attacks and then we see if you share those same gene variants, there are weights given to each of these gene variants, and then you come up on a scale of low, medium or high risk.
“I’m really excited what we have in the pipeline with this sort of scoring ... incorporating that with the coronary calcium score and putting it together and getting a global integrated risk score”
But we’re not able to give specific numbers just yet, other than relative risk or absolute risk just because our dataset wasn’t large enough to do that. But what we’re developing right now, you’d essentially get a polygenic risk score or polygenic risk assessment that takes into account these genes associated with familial hypercholesterolaemia, but also other ones that on their own don’t dramatically increase your risk, but in aggregate if you take 20 or 30 of them together they can tilt you one way or the other.
So that’s actually the really exciting part, using polygenic risk scales and scores and building those models out. And we’re just at version one of this I’m really excited what we have in the pipeline with this sort of scoring and also incorporating that with the coronary calcium score and putting it together and getting like a global integrated risk score. So that's where we’re headed, but right now I’d say these polygenic risk scales can tell you you’re a little bit more like people with heart attacks or you’re a little bit less like people with heart attacks but it doesn’t give you an actual number just yet.
LB: That’s really clear and you’ve mentioned version one a few times so it’s clear that one of the things we need to do is get more and more people to come through the Health Nucleus and share their genetic information and family history etc.
One of the things I get really excited about and really enjoy in my visits to the Health Nucleus is going into the MRI machine. I think that’s one of the coolest things you guys do, I love picking the scene, the light color, the music, the things to look at. It’s really awesome.
Q: What kind of data will you be pulling out of the MRI scans and what will you be using it for? Besides the heart analysis and some of the cancer detection, which we already discussed. What will be showing up in that data and what will you use it for?
I’ve split this interview into FOUR parts, due to its length! Part 3 will drop next week!
Previous Post: Part 1
Note: the Health Nucleus has recently appointed a new Medical Director - Dr. Pamila Brar. Dr. Duchicela has transitioned to a role as full-time physician at the Health Nucleus, working directly with patients to optimise their healthcare!










Follow me on Twitter for the latest #Longevity news!
-
 RT @rebeccavziegler: The cryonics payoff matrix. Choose wisely my friends. https://t.co/l1rzsmOC2w
RT @rebeccavziegler: The cryonics payoff matrix. Choose wisely my friends. https://t.co/l1rzsmOC2w -
My rate of aging: 0.79 It’s the new street cred What you got? https://t.co/aHzWHAfCnD https://t.co/L3rZC4QFN2
-
It’s official - I’m co-producing and hosting a new #longevity docuseries, and will begin shooting in a few months… https://t.co/wLGqRrBfbp
-
“The #longevity segment opened my eyes to the groundbreaking advances in biotechnology, health, and wellness. The i… https://t.co/F8YB7PAeMW
-
I’m completely mindblown by what AI has done over the past 3-6 months, and it continues to accelerate… https://t.co/hh0JslucRg
-
Longevity legends take on many shapes and sizes https://t.co/X9vGa7gvOe
I post related #Longevity content to Instagram as well, follow me @nickengerer













FDA & TGA DISCLAIMER
This information is intended for educational purposes only and is not meant to substitute for medical care or to prescribe treatment for any specific health condition. These blog posts are not intended to diagnose, treat, cure or prevent any disease, and only may become actionable through consultation with a medical professional.

3 Technologies for Monitoring Heart Health
Three heart health technologies looking after your ticker
Monitoring heart health is a top priority. When it comes to listing your vital organs - those needed most for your overall well-being and the joy of being alive, the heart comes up at the top of the list (along with your brain, liver, kidneys…).
It should be at the top of the list for all longevity enthusiasts keen to look after their long-term health. But what technologies are accessible and valuable for this purpose?
Heart Health and the EKG
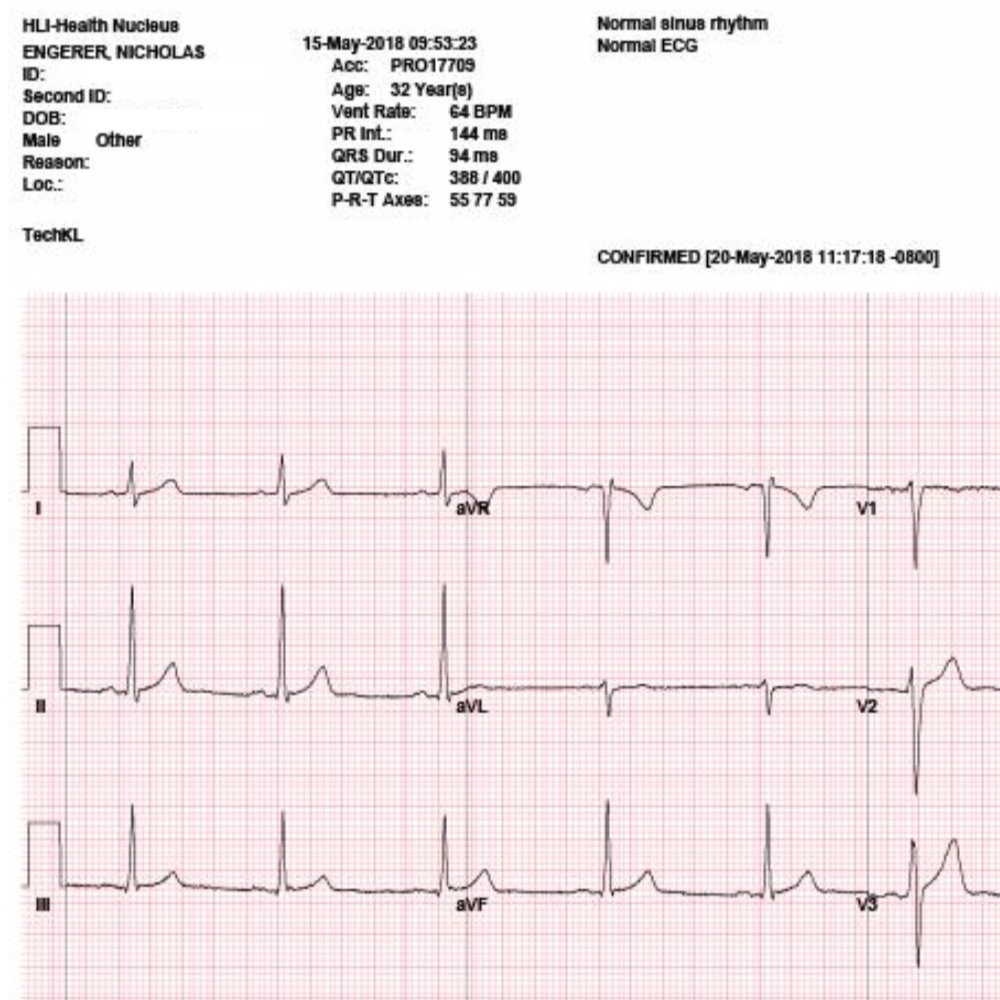
Health Nucleus EKG results for Nick were all fine and dandy!
An EKG is short for ‘electrocardiogram’. The EKG is on the frontlines for assessing heart health, and is particularly valuable in the case of an ongoing heart attack.
An EKG is completed by checking the electrical activity of the heart by attaching several small sticky electrode pads to your arms, chest and legs.
The EKG provides the following information:
Analysis of blood flow to your heart muscle
The electrical signals of heart rhythm
A first line of detection for abnormalities
Detect electrolyte imbalances
What’s fascinating about EKGs is how accessible the technology has recently become.
Perhaps the biggest impact on accessibility of this test has been made possible by the Apple Watch, for which Series 4 and above have EKG capabilities
But the Apple Watch is not alone! Several other ‘test at home’ technologies are also available. “Emay” is another technology brand which has entered the space.
They have an impressively compact and slick device, which we personally prefer over the Apple Watch due to its lower cost and dedicated function (does an iMessage on your wrist help your heart health?).
Don’t get confused about the “ECG” term, EKGs and ECGs are the same test.
Heart Health and Cardiac MRI
In an earlier post we discussed the merits of full body MRI and cardiac MRI.

Example of Nick’s cardiac MRI findings. Note the very particular measurements of the heart anatomy.
MRI stands for magnetic resonance imaging. A heart or cardiac MRI looks into the structures of the heart and its neighbouring blood vessels in great detail.
A Heart/Cardiac MRI is used to diagnose/check for:
early signs of heart disease
assess the the heart for any signs of damage
detect any imminent heart failure or defects
assess inflammation of the membrane lining the heart
While you certainly can’t perform a cardiac MRI at home, you can work with organisations like the Health Nucleus or a specialist to have these tests completed.
Heart Health and THE ZIO

Wearing the Zio
Two weeks of detailed heart-rate data, under all conditions - exercise, rest, day-to-day activity. Including tracked events where Nick pushed the button for closer inspection in the report (see below).
As a part of Nick’s preliminary Health Nucleus visit, he was sent away with a small stick-on device called a ‘Zio’ that he wore for two weeks.
The Zio watches heart-rate in great detail and and includes the ability for the user to track events of interest by clicking the device.
Nick noted he ‘clicked’ the button on a few events where his heart-rate seemed to pick-up and beat hard after lying down in my bed.
He’d actually noticed these events for most of his adult life, and had passing concern about what that indicated about my heart/body health.
Those events have now been analysed in great detail and revealed no underlying heart driven worries.
The Zio device is attached with a gentle adhesive which did not cause any skin irritation.
Beyond having to ‘bag’ the device in order to take a shower (covering it with plastic and tape), it is a very easy device to manage.

Notes from Nick: “Those ‘Black dots’ are regions where I clicked the button for closer inspection. These were events where I noticed my heart-rate seeming to pick-up, or be more noticeable after lying down in my bed.
I’d noticed these my whole life - now I know they have no underlying heart driven worries and can rest easy :)”

Zio IRhythm overall report after two weeks
Nick’s Zio report. 175bpm during an intense workout. 52 bpm minimum recorded during the overnight.




FDA & TGA DISCLAIMER
This information is intended for educational purposes only and is not meant to substitute for medical care or to prescribe treatment for any specific health condition. These blog posts are not intended to diagnose, treat, cure or prevent any disease, and only may become actionable through consultation with a medical professional.