
Premium longevity healthcare - Interview with Health Nucleus Part 4
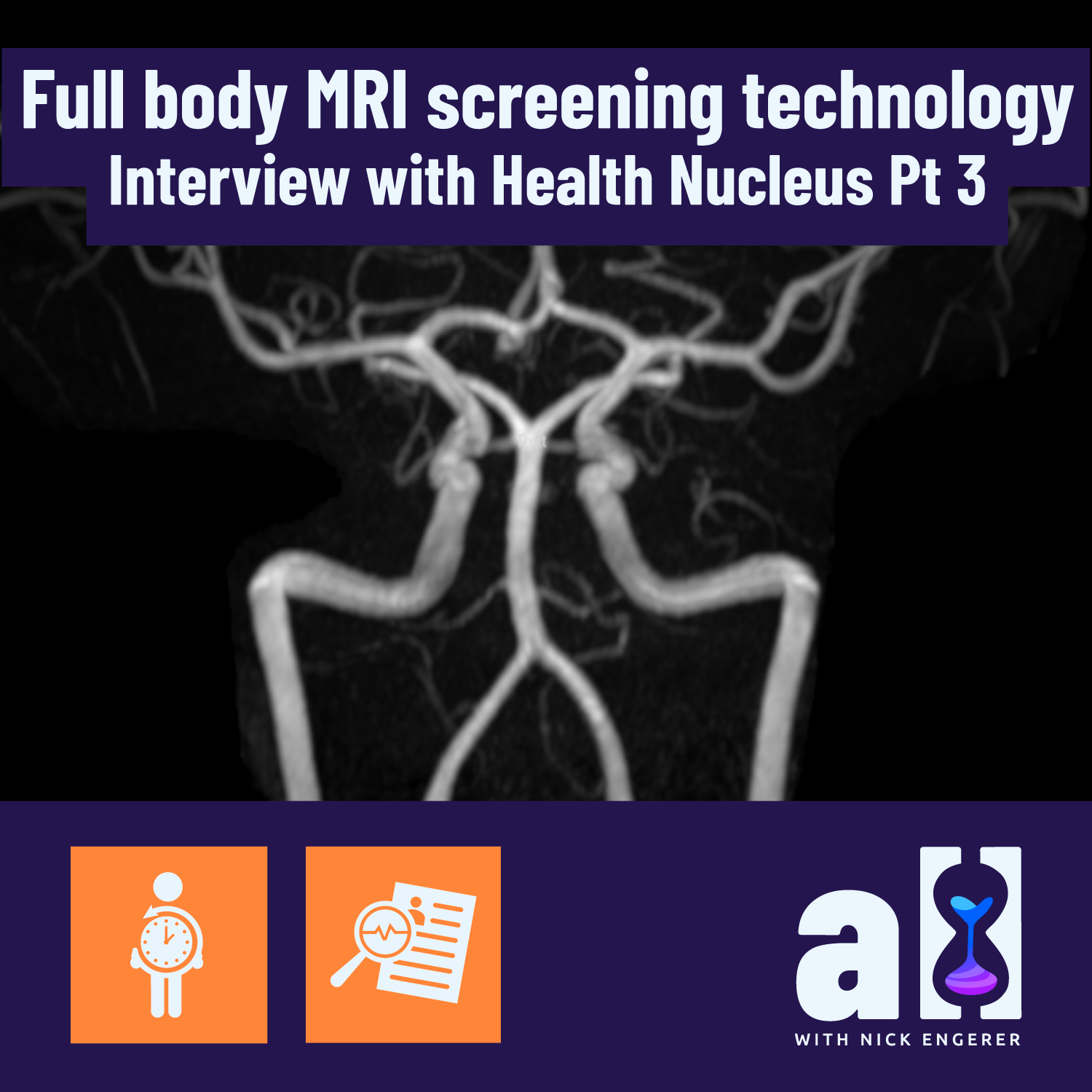
Full body MRI screening technology - Interview with Health Nucleus Part 3
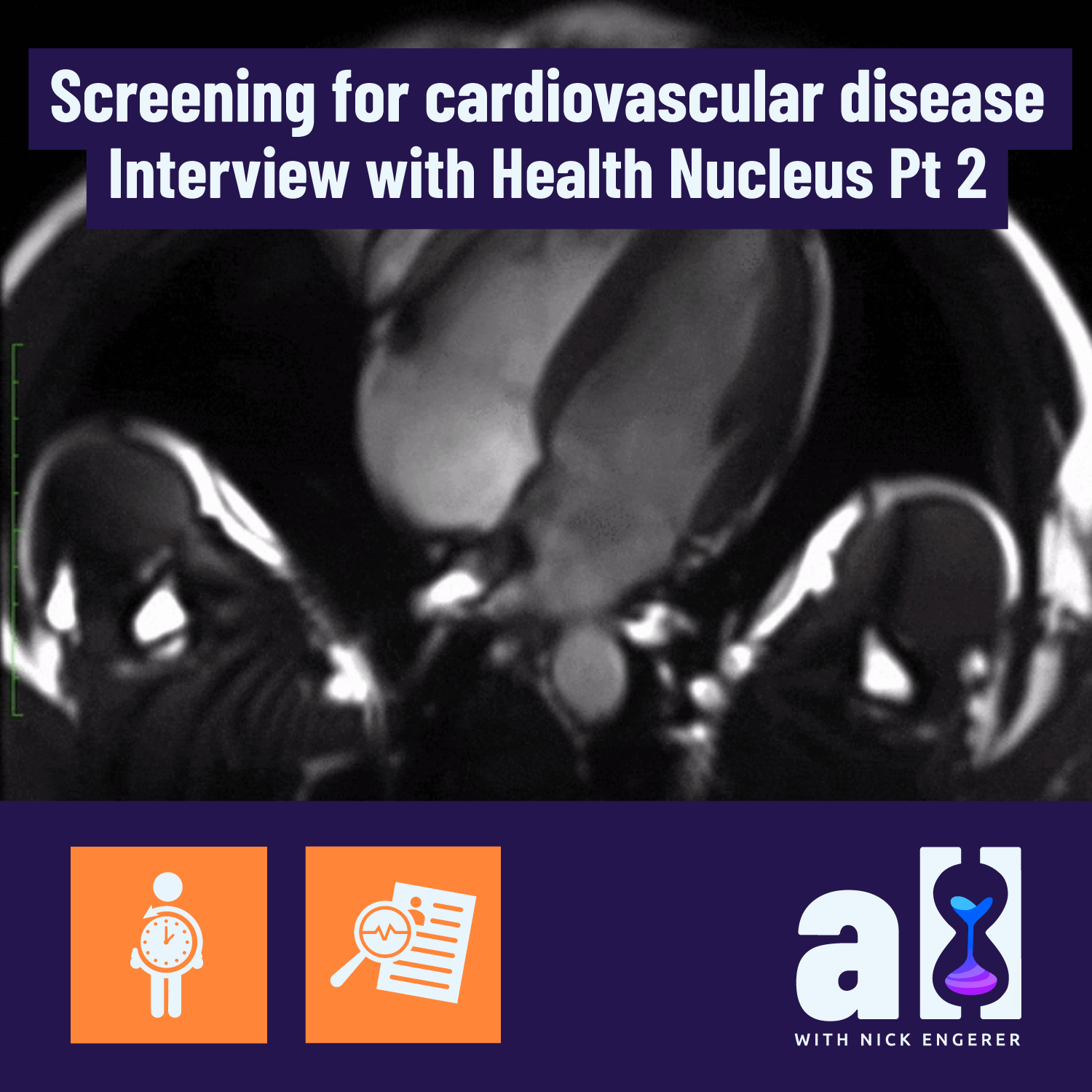
Screening for cardiovascular disease with MRI and CAC - Interview with Health Nucleus Part 2

Early cancer detection and big data - Health Nucleus interview Part 1

Full body MRI data: health screening of the brain, heart and abdomen
What is a 3D full body MRI and what did I learn from completing one at the Health Nucleus in San Diego?