
Premium longevity healthcare - Interview with Health Nucleus Part 4
In this post you’ll learn about:
The personalised nature of a Health Nucleus visit
A vision for getting tens to hundreds of thousands of patients through this proactive healthcare provider
Why Dr. Duchicela likes the Longevity Blog :-)

One of my favourite aspect of a Health Nucleus visit is the number of experts reviewing my medical data, to guide my health outcomes. Here I am getting my blood drawn in January 2020.
Dr Duchicela: Dr Duchicela:
[laughs] There’s a lot of people let’s just say, with the caveat being that everything is very private and HIPAA compliant, but in terms of clinicians, it’s a physician like myself trained in family medicine and preventative medicine who would be looking over your report results, you’ll have at least one radiologist and a lot of times two radiologists because we do double checks where they check each other, which I think is good practice. You’ll have a cardiologist looking at your heart scan, the cardiac MRI is read by a cardiologist and not the radiologist and then with the genetics you will have the clinical genetics team reviewing any significant findings that you had and if there is something that was flagged, a lot of times what they’ll do is delve into the clinical history a bit more and talk with myself or one of the physicians.
So by the time your return of results session comes around you’ll have a lot of different clinicians looking at your data and analysing your data and there’s wide communication between the teams as well. If there is a significant finding we will also have a genetic counselor as part of the return of results session as well. A lot of different clinicians just for one person which is pretty amazing, I think it’s pretty cool to be honest that you have so many different disciplines involved in your care, but you kind of need to just because we look at some many different modalities.

Speaking of genetics data - I recalled fondly this Longevity Blog post exploring haplogroups and ancestral DNA.

Phlebotemy in action! It had been a few posts since I mentioned how gorgeous the staff at NextHealth are!
LB: Q: If you had to estimate the size of the clinical genetics team, how many folks would be looking at the data - it can be a range.
Dr Duchicela: We have two or three people at least looking into any significant variants or looking into something in the family history that was flagged, and they will do a deeper dive session into it. Two or three clinicians on that team that are dedicated to this.
LB: Q: And then in terms of other folks I’ll work with, there will probably be a phlebotomist, there might be some other nurse staff.
“we are developing is a follow up program where we have a nurse practitioner or a physician reach out every so often at different intervals and say ‘hey, how’s it going?’”
Dr Duchicela: A phlebotomist, a medical assistant, you’ll interact with all the different techs, there’s a different tech for the CT scan, a different tech for the MRI, a nurse for the balance tracking and body metrics collection, and what’s really exciting and what we’re hiring for right now and for the future we’re starting to develop a longitudinal program and we’re going to be hiring a nurse practitioner to actually check in with patients over time.
Right now I think one of the main criticisms of our testing is you come in for an evaluation, you get the testing done, you get the results back and then it’s almost like I’ll see you next year or I’ll see you in two years and there’s not a lot of touch points in between that. So what we’re going to be developing is a follow up program where we have a nurse practitioner or a physician reach out every so often at different intervals and say hey how’s it going, did you follow up with this particular test, we talked to you about this finding on your MRI did you ever go in and get that checked out with the specialist. I think it's just good care to do that and I think it hopefully reengages the patient too and gets them to keep thinking about their health.
It’s really easy after you get your results back you go hard for a month or two or three afterwards, cut out refined carbohydrates and start exercising every day and giving up smoking or cutting back on wine. But after three or four months that motivation kind of wears off which is just normal human nature. So what I would like to see happen more is that we have some sort of continuity program where we reach out throughout the year and say hey how are things going? Let’s check in. How can we support you?
LB: Count me in!
Q: There’s a lot more than just the clinicians and nurses you’ve mentioned behind the scenes at Human Longevity Inc, I know you have an R&D staff who are developing new analytics and new reports. I’ve actually met with some of them and discussed some of the new reports HLI is developing. What does that team look like? And what are some of the exciting things they are working on at the moment
Dr Duchicela: Yeah we have a lot of engineers, we have people who are specialists in imaging and in post processing imaging, machine learning scientists. In terms of what they’re working on, there’s two categories of goals with our products. We want to create products that are firstly accurate and second we want them to be accessible to the lay person, to the general consumer and we also want them to be accessible to physicians too who maybe aren’t trained in genetics or in precision medicine testing. We are continually trying to evolve our reports to make them easier to understand. It is a challenge, to be completely transparent, to take all of this information and to condense it and put it into an easily digestible report.
“We have an imperative to scale and to make this more affordable for people”
It’s hard to do and I think our initial iterations of this, we were essentially writing reports by PhD’s for PhD’s, which I felt we had to change, we needed to make it more accessible. That’s one aspect, how do we visualise the data differently, using the webportal to make it more apparent where people could enact change. The second aspect of that is what is the value of getting the testing through us versus an MRI somewhere else or genetic testing somewhere else and putting it all together on their own. I think it's really the analytics, taking these different modalities building these algorithms that are essentially like a crystal ball and doing it for the top five diseases and being able to dynamically say if you stop drinking alcohol or cut back on smoking your disease risk for alzheimers will go down by X percent. Kind of knowing that and having those numbers and validating them and also getting them FDA approved, that is kind of what we’re looking at in terms of the pipeline.
Side Note: All-up, I estimated that more than 15 unique staff review results or directly support the technology used to asses a patient’s data for a given Health Nucleus visit. Now that’s personalised medicine!

“I believe we have a chance to make 100 years old the new 60… for you, your family, friends and colleagues.” - the transformative purpose of HLI is to make 100 the new 60, and make the technology broadly accessible. Read more on co-founder Peter Diamandis’ Blog
And in scaling this, how do we offer this testing at a lower price point? With the MRI in particular, we’re looking at a lot of things with the MRI and that makes the scan time longer, so how do we develop software that makes the scan time less to make it more accessible to people and still get really really good data from it. So all those things we’re working on trying to optimise. We have an imperative to scale and to make this more affordable for people and we want to provide better insights based on the integrated data and building the models for that. That’s the exciting part about it and that’s what we're going to be focusing on in the three to five year range.
LB: Great! Keegan, thank you for taking the time to talk to me about this, it’s been fascinating, exciting and very enjoyable. I am excited that you’re in a leadership position at the Health Nucleus and have the vision and passion for this topic that you do. That’s fantastic for everyone that gets to come through the Health Nucleus.
Dr Duchicela:
That’s kind of you to say. I feed off the enthusiasm of the patient’s who come through. Just like yourself, we get some really interesting people coming through, people who are passionate about optimising their health. They really want to know their data and they want to take not only the insights that we can provide but they also want to take their data and make their own insights into it as well and they kind of just run with it and I think it’s fascinating and fun to see and it’s encouraging to see that people are so engaged with their health, that’s what I feed off of, that kind of enthusiasm, especially the early adopters like yourself who know and see the value of this.
We know that this sort of testing is going to be here and be ubiquitous in the next ten years once the price point comes down and we have the opportunity to educate more people about it and the testing becomes better. It’s really exciting to see we have a community now that’s growing around the types of testing that we’re doing and precision medicine in general so I think it’s an exciting time to be a part of it and to see where it goes.
LB: You mentioned this is version one of the algorithms and the need for more data over time to improve them.
Q: How many people do we need to have come through the Health Nucleus to make it possible for your team to have the data they need to make that crystal ball possible?

We discussed polygenic risk scores in Part 2 - find it here.
Dr Duchicela: I think we’re almost there to be honest. They’re already in development of these models right now and we use not only our data sets but we do derive from external data sets like the UK Biobank and other things that feed into these models. But for our next versions of the reports for these polygenic risk scales, we actually do have enough numbers now to give relative risk for a lot of conditions, which will be very helpful for knowing more about your health.
[Our target enrolment is] 100,000 people to do this type of deep analysis on. I think we will definitely be able to create models with less than that, but also using external data sources as well. So, stay tuned. I think in the next few months, they want to come out with these new versions of polygenic risk scales with relative risk and then validating more of these global disease models for diabetes and alzheimers and certain cancers and the non-diseased as well. So yeah we’re almost there with getting these crystal ball algorithms. Which is really exciting!
LB: So 100,000 people, that’s our target! How many more do we need?
Dr Duchicela: [Our current target is] 100,000. We want to build 10 of these centers around the world and we want to drive a certain number per year through. To date, we have had 5,000 people come through and with that number and with such a deep data set that we have, we’re starting to make some really really good models.
LB: Great, well good on those 5,000 people for helping to make this possible. And I will be doing my part to help you get 95,000 more!
Q: Anything more you want to add?
Dr Duchicela: I love your passion for this and I like your blog!
Note: the Health Nucleus has recently appointed a new Medical Director - Dr. Pamila Brar. Dr. Duchicela has transitioned to a role as full-time physician at the Health Nucleus, working directly with patients to optimise their healthcare!
Follow me on Twitter for the latest #Longevity news!
-
 RT @rebeccavziegler: The cryonics payoff matrix. Choose wisely my friends. https://t.co/l1rzsmOC2w
RT @rebeccavziegler: The cryonics payoff matrix. Choose wisely my friends. https://t.co/l1rzsmOC2w -
My rate of aging: 0.79 It’s the new street cred What you got? https://t.co/aHzWHAfCnD https://t.co/L3rZC4QFN2
-
It’s official - I’m co-producing and hosting a new #longevity docuseries, and will begin shooting in a few months… https://t.co/wLGqRrBfbp
-
“The #longevity segment opened my eyes to the groundbreaking advances in biotechnology, health, and wellness. The i… https://t.co/F8YB7PAeMW
-
I’m completely mindblown by what AI has done over the past 3-6 months, and it continues to accelerate… https://t.co/hh0JslucRg
-
Longevity legends take on many shapes and sizes https://t.co/X9vGa7gvOe
I post related #Longevity content to Instagram as well, follow me @nickengerer













FDA & TGA DISCLAIMER
This information is intended for educational purposes only and is not meant to substitute for medical care or to prescribe treatment for any specific health condition. These blog posts are not intended to diagnose, treat, cure or prevent any disease, and only may become actionable through consultation with a medical professional.
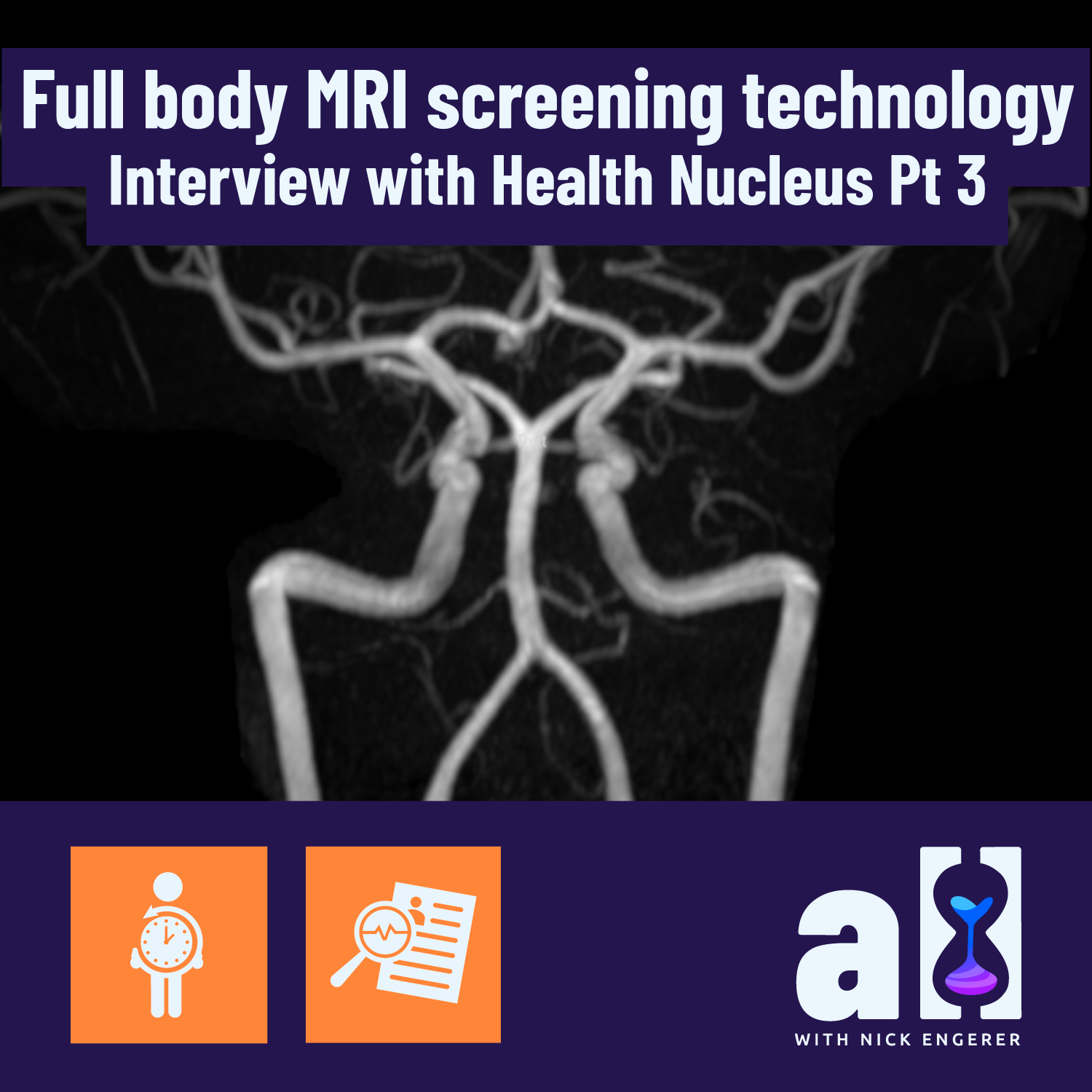
Full body MRI screening technology - Interview with Health Nucleus Part 3
In this post you’ll learn about:
The power of Health Nucleus MRI algorithms (e.g. early detection of brain aneurysms or quantifying visceral fat levels)
Same examples of how multiple Health Nucleus visits enable deeper personalised analytics
How the Health Nucleus is prevention focussed, rather than on optimisation (but that’s a good thing!)
Part 3 - MRI analytics & health optimisation
Be sure to read Part 1 and Part 2!
Longevity Blog (LB):
Q: What kind of data will you be pulling out of the MRI scans? Besides the heart analysis and some of the cancer detection, which we already discussed. What will be showing up in that data and what will you use it for?

The blood vessels of my brain as revealed by Health Nucleus MRI data. Aneurysm free and healthy :)
Dr Duchicela: I think primarily it’s used for detecting the big things that we don’t want to miss that we really want people to know about early on, so things like cancer or aneurysms. With the post processing that they do on it, they’re able to reconstruct vasculature and vessels to look for aneurysms, even without using contrast which i think is really neat.
And then we have these different imaging biomarkers, so for Alzheimers we do hippocampal volume assessment where we look at the volume of the hippocampus and the ventricles surrounding them, and essentially see how do you compare to a healthy peer group? Are you a little bit lower or a little bit higher in these volumes, which correlates with Alzheimer’s risk. That’s one aspect.

At left, my visceral fat levels are highlighted by Health Nucleus MRI algorithms. Visceral fat is known to increase with age, and increased levels are risk factor for many diseases.
With MRI we also get the body composition like visceral fat levels, liver fat levels, liver iron levels, and muscle composition. What we’re doing with the MRI data is essentially training algorithms to better detect the sorts of cancers that traditionally you can’t detect with a non-contrast MRI, one we are working on right now is pancreatic cancer. We’ve developed a screening tool to use in MRI for pancreatic cancer and we’re in the process of validating it which is really really exciting. But that will just add to the overall comprehensiveness of the scan and of the experience, so yeah there’s lots of different things we get from the MRi, it’s pretty amazing how much data you can get from it and how much you can start to train these algorithms.
LB: Diving deeper into MRI analytics - I have a full body scan from May 2018, I’m soon to have another scan from January 2020, and plan to continue to do these scans every 12 to 24 months depending on my travel schedule, so you’re going to get a bit of a time series going with the data.
You’ve talked about disease risk and obviously we’ll keep assessing those things but in terms of somebody who’s trying to optimise, like myself who’s a bit of a biohacker or maybe an athlete who’s thinking about their performance and their muscle composition…
Q: What kind of optimisation intelligence could we derive from MRI data over time?
“If you come back multiple times, year to year or every two years, we can trend many things and see how you’re doing. ”

MRI analytics of muscle mass. At left, my colour coded leg muscle groups in May 2018. At right, January 2020. I added 1.3L of muscle mass during that time. Note: the pictured images are from a slightly different ‘slice’ of the data.
Dr Duchicela: I would look at the imaging biomarkers, looking at the visceral fat measurements and subcutaneous measurements that we get and quantifying and trending that. The scanner software automatically marks out where your subcutaneous fat is, where your visceral fat is, we can trend your liver fat measurements, your liver iron measurements and then obviously your muscle composition too and where you’re distributing your muscle.
If you come back multiple times, year to year or every two years, we can trend many things and see how you’re doing. Some people, even if their metrics are “within a normal range”, they want to get them better, and so when you have such an accurate test like the MRI you’re able to make that quantification, you’re able to make those comparisons versus for example other machines out there that measure your visceral fat too and kind of trend it, but really MRI is pretty darn accurate for that and one of the most accurate assessments available, so if you really want to know the numbers and get that in addition to your cancer assessment and your aneurysm assessment, I think MRI is the way to go.
LB: That’s really spot on in terms of the answer I was looking for, one thing I’d like to prompt you on…
Q: Is there opportunity to analyse the strength or flow volumes of the heart from your MRI data?

Dr Duchicela: We can see that your ejection fraction or how much blood you’re pumping out of your heart changes over time, now the question is does that actually translate into performance increases? We don’t necessarily think so for healthy individuals, because there’s lots of other things, like how fast your heart rate is going etc. So I would say not yet, I see where you're going with the question in terms of, could it be used to measure and trend athletic performance, not only for elite athletes, but for lay people who want to really maximise their athletic performance. I don’t think we’re there yet and I don’t think that’s necessarily the overall goal of this test. I think there’s a different series of tests that probably could do better than just the MRI for athletic performance trending and monitoring.
LB: Q: Are there any unique Health Nucleus tools that could be applied to assessing athletic performance and/or optimisation?
Dr Duchicela: I think with genetics we’ll start to get more information on that. There's already genetic predispositions to things like muscle tissue fibers and that sort of thing. What I would want to do as a medical director is to try to delve more into that and gather information on athletic history and get these metrics like VO2max and mile time etc and then start to work with the genetics to see if there are any predictors where we could make some correlations. That I think would be really exciting to do at some point in the future.
“I’m really excited what we have in the pipeline with this sort of scoring ... incorporating that with the coronary calcium score and putting it together and getting a global integrated risk score”
LB: Yeah I agree with you that it would be very exciting, and again it’s not your current focus, but I was curious to ask a few questions on the topic of optimisation, so thanks for that.
One of my big outcomes from my last visit to the Health Nucleus was a ‘prescription’ for cardio exercise and to increase my muscle mass on direct guidance from one of your doctors. I took that exceptionally seriously and have been dedicated to cardio fitness routinely since that time. So I’m really curious what you think might be evident in terms of one’s biometrics and data coming from their visit to help one measure their improvement in fitness over time.
Q: You’ve talked about MRI, and a bit about genetics, what else in there might show up in this visit compared to last time if I’ve done a good job at that cardio and exercise routine?
“ the best areas to look for changes and improvements would be in your imaging biomarkers, your core lab tests for metabolic biomarkers, lipids, a1c and fasting sugar. ”
My blood lipid panel over time; some great changes in between my first Health Nucleus visit (May 2018) and my second (January 2020).
Dr Duchicela: Yeah we’ve already mentioned the imaging biomarkers like your body composition, your liver fat level, those will definitely change with lifestyle change for sure, and then I would look at your traditional blood markers. You’ve probably already been measuring those, but making sure your [Hemoglobin] A1c is good, as well as your fasting sugars and your cholesterol numbers. In terms of trending data, that’s the kind of metabolic panel we would do. We can’t trend genetics so much, so I would say the best areas to look for changes and improvements would be in your imaging biomarkers, your core lab tests for metabolic biomarkers, lipids, a1c and fasting sugar. That’s where you’d probably best be able to see improvement and change.
LB: Cool, thanks for diving into that. And in terms of the genomic data that we’re pulling out, Q: what information in there will be actionable for somebody who wants to optimise? There’s examples of the ways you might metabolise certain precursors to vitamins, such as not being a good converter of beta carotene to retinol in the blood or the MTHFR mutation for methylation.
“It’s probably too early to hang your hat on these variants that tell you to eat a certain food or to do something very specific in terms of lifestyle unless you have one of these obviously high risk genes”
Dr Duchicela: Yeah I think that’s kind of the challenge with the genetics, the focus of the company from what I’ve seen so far is more on the hidden health risks with these high risk cancer genes, high risk cardiovascular disease genes or neurodegenerative disease genes.
In terms of optimising genetics, from what I’ve discussed with the clinical geneticist here and the genetics team, It’s probably too early to hang your hat on these variants that tell you to eat a certain food or to do something very specific in terms of lifestyle unless you have one of these obviously high risk genes, these monogenic findings. But I think it’s an area of consumer interest, what we're hearing from a lot of people is they want more specific lifestyle modifications based solely off genomics. I think that our genetics team needs to be a little more convinced that there are really good actionable things there.
It’s also a matter of prioritisation of where we put our resources, do we want to be more of a lifestyle service versus more of a medical service that’s catering towards physicians and the medical community? I think we’ll always have tension on where the focus should be. Right now the testing is looking for high risk medical issues that we can intervene on, like is there a BRCA mutation or a gene that puts you at high risk of colon cancer?
I am curious to know and to see where the science takes us with more of these lifestyle influenced variants, but i would say for right now for our testing [optimisation] is not one of the big focuses - we really want to try to prevent disease first and build off of that and then delve more into and put more resources toward lifestyle genomics.
LB: I think that that focus area is apparent from the way your suite of testing and reporting is arranged. In my view, everybody needs to be taking advantage of these proactive aspects of medical technology before thinking about health optimisation. You’ve got to take care of the core risk and any acute issues first, in order to maintain your wellness. So I don’t think that focus is misplaced at all. It’s intriguing to hear that your team is interested and noting increased demand for this sort of individual attention. I certainly think that that’s a growing market as well.
“what is the patient’s goal?”
Dr Duchicela: Totally. There’s a lot of companies out there that will do some direct testing and tell you exactly what to eat or avoid this food based off of you having this variant. I think we want to be a little bit more careful with that just because you really have to look at things holistically. I don’t think we really want to say - stop eating cucumbers based off your genetics, we really want to take into account what the patient’s preferences.
Like i was mentioning before with the wine example, really what is the patient’s goal, is their goal to have a super restricted diet so they can live forever, or is it to enjoy time with their family, or to be able to do a certain activity better, so I hesitate to hang everything onto genetics and dictate lifestyle just based on your genetics. We really want to develop something that's more holistic.
LB: That’s where the physician comes into the picture - in having a relationship with them that’s ongoing and aligned with your personal goals and values. I think it’s excellent you’re even mentioning personal values and thinking about them as a physician.
One of the things I think is totally rad is that - I’m sitting here interacting with you, I’m going to be talking to a doctor and several team members on my visit next week - Q: I was curious if you could remind me of how many medical professionals will be interacting with me directly or with my data as an outcome of my Health Nucleus visit?
I’ve split this interview into FOUR parts, due to its length! Part 4 will drop next week!
Previous Posts: Part 1 - Part 2
Follow-up Posts: Part 4
Note: the Health Nucleus has recently appointed a new Medical Director - Dr. Pamila Brar. Dr. Duchicela has transitioned to a role as full-time physician at the Health Nucleus, working directly with patients to optimise their healthcare!
Follow me on Twitter for the latest #Longevity news!
-
RT @rebeccavziegler: The cryonics payoff matrix. Choose wisely my friends. https://t.co/l1rzsmOC2w
-
My rate of aging: 0.79 It’s the new street cred What you got? https://t.co/aHzWHAfCnD https://t.co/L3rZC4QFN2
-
It’s official - I’m co-producing and hosting a new #longevity docuseries, and will begin shooting in a few months… https://t.co/wLGqRrBfbp
-
“The #longevity segment opened my eyes to the groundbreaking advances in biotechnology, health, and wellness. The i… https://t.co/F8YB7PAeMW
-
I’m completely mindblown by what AI has done over the past 3-6 months, and it continues to accelerate… https://t.co/hh0JslucRg
-
Longevity legends take on many shapes and sizes https://t.co/X9vGa7gvOe
I post related #Longevity content to Instagram as well, follow me @nickengerer
FDA & TGA DISCLAIMER
This information is intended for educational purposes only and is not meant to substitute for medical care or to prescribe treatment for any specific health condition. These blog posts are not intended to diagnose, treat, cure or prevent any disease, and only may become actionable through consultation with a medical professional.
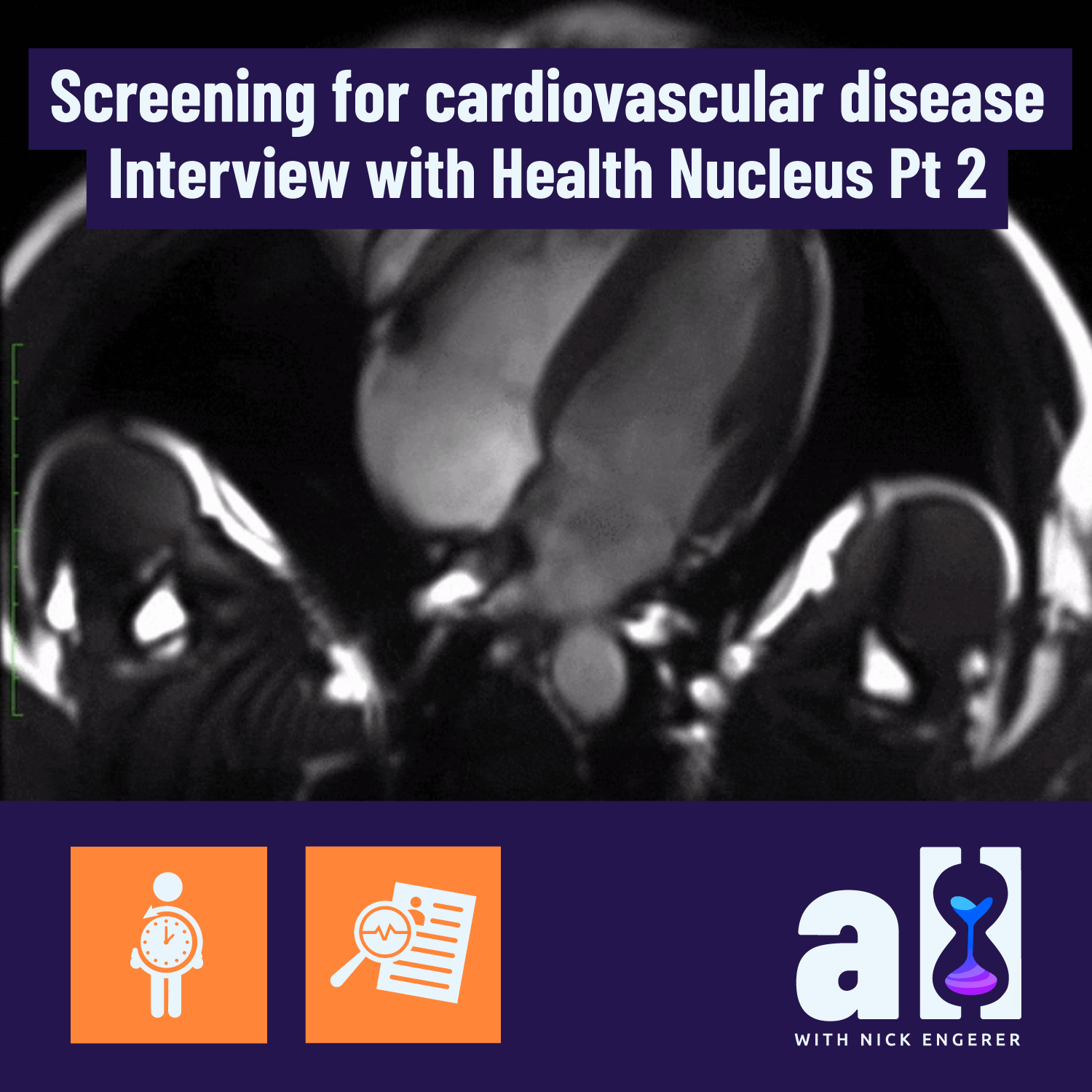
Screening for cardiovascular sisease with MRI and CAC - Interview with Health Nucleus Part 2
In this post you’ll learn ABOUT:
Health Nucleus tools for assessing cardiovascular disease risk
The role of the Coronary Artery Calcification (CAC) score in assessing risk, particularly for younger people (30s, 40s)
How CAC scores might influence statin use
The limitations of MRI data in assessing risk
How genetic risk factors might influence risk
Combining imaging data, genetic factors and blood tests to further clarify risk
Part 2 - Cardiovascular disease
Be sure to read Part 1!
Longevity Blog (LB):
We’ve talked a little bit about cancer. Another big killer whose risk is a function of how old you are and a number of genetic factors is cardiovascular disease and in particular atherosclerosis.
I understand my risk as a man in his thirties is low for an acute event now, but the disease risk grows with time as the result of a decade on decade buildup of plaque, inflammation and wear and tear on the arteries…
Q: So how does coming to the Health Nucleus help inform someone about how their risk might change as they get older? What could a young person do using this information to minimise their risk of atherosclerosis and cardiovascular disease?

Coronary Artery Calcium Scoring. Credit: Cleveland Clinic
Dr Duchicela: Yeah that’s a great question. So in terms of cardiac assessments, one of the most powerful ones that we do here is the coronary calcium score. This is looking at calcified plaque buildup in the arteries of your heart. Essentially, the more plaque you have the higher your risk is of a heart attack.
You’re right, for someone in their thirties, who’s young, who is otherwise healthy, the chances of you finding plaque are low. Based on the general standard of care in the community, we wouldn’t be getting a coronary calcium score on somebody who’s 35 years old or younger. But here, because we’re under a research protocol, we have a little bit more leeway to push the boundaries in terms of testing in groups that may not otherwise be traditionally tested.
“we’re finding that actually about 15 to 17% of individuals around the age of 40 to 45 or younger actually have significant plaque build up. ”
And so for the coronary calcium score for example we are able to do it on a 35 year old, or 36 year old and we’re finding that actually about 15 to 17% of individuals around the age of 40 to 45 or younger actually have significant plaque build up. So we are probably missing a good amount of people out in the community who have atherosclerosis and calcified plaque in arteries of their heart which will predispose them to heart disease.
So when you come here to Health Nucleus and you if you meet the age requirement of 35 years or older (that’s what do here for the coronary calcium score), you’ll see what your plaque level, your score is, and then we will compare you to other people your same age and gender. So you get a sense of how you stack up to a healthy peer group as well and based on that, we take that into account with your cholesterol numbers and so, let’s say you have high cholesterol numbers, your LDL is elevated and your doctor is trying to push you to be on a statin or a cholesterol medicine.
If you get a coronary calcium score and your score is 0, there’s no calcified plaque seen, then you actually have a pretty good case to make that you shouldn’t be on a statin just yet . A lot of men and women come through here and their doctors are pushing and pushing them to be on a statin because their cholesterol is on the higher side, and we scan them and we get their coronary calcium score and it’s zero or very low that actually is pretty powerful in that it makes it not as urgent to be on a statin and you can talk more about lifestyle modifications and the diet, the exercise and maybe hold off on that statin for awhile longer.
A lot of men and women come through here and their doctors are pushing and pushing them to be on a statin because their cholesterol is on the higher side, and we scan them and we get their coronary calcium score and it’s zero or very low
LB: That’s a really clear answer Keegan, thank you for that.
Q: Could you comment a little bit on what the Health Nucleus can do with the MRI technology in terms of cardiovascular risk?
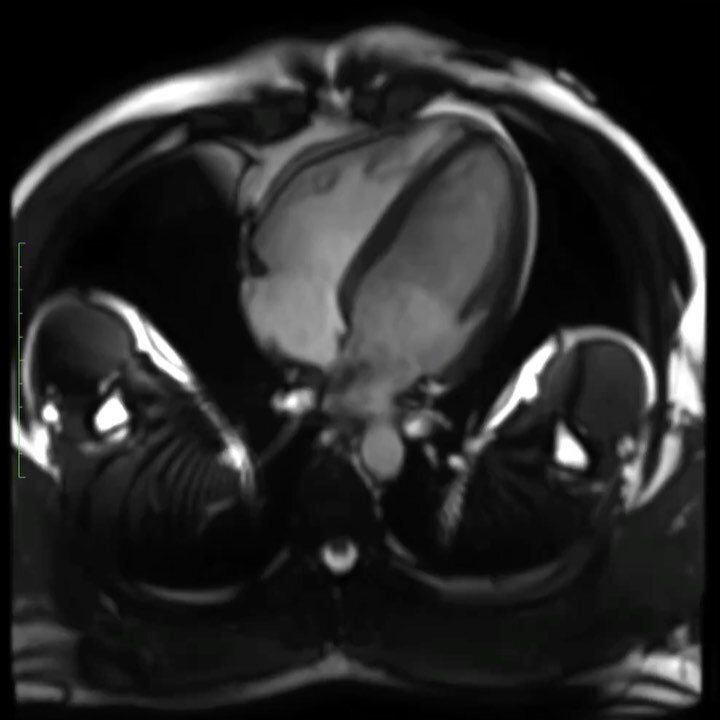
My heart beating, as observed by the Health Nucleus full body MRI scan and post-processing technology.
Dr Duchicela: For heart attack risk you get most of the assessment from the CT scan and the coronary calcium score. From the MRI what we’re doing is more structure of the heart so this is like what the chambers look like, how large the chambers are, or if they are hypertrophied or thickened because of high blood pressure or if it’s not pumping as well as it should be, like the ejection fraction is low because of early congestive heart failure or some sort of other heart failure. That’s what we get from the MRI. The MRI is more structural. It can find congenital abnormalities of the heart sometimes too, where as the CT scan, the one that involves a little bit of radiation, that is more for heart attack risk.
LB: That’s a good differentiation. Thanks for taking the time to answer that. And so in terms of a young person coming in, you’ve mentioned this kind of threshold of 35 years or older to do the calcium score, I don’t meet that criteria quite yet, but I’ll certainly do it when I get to that point.
Q: What other Health Nucleus tools can sit alongside the diagnostic imaging tests (MRI, CAC score) which can help a young person evaluate their lifetime risk of atherosclerosis?

Dr Duchicela: In terms of genomics, there are some genetic markers that predispose you to very high levels of cholesterol, that would be picked up not only in the blood screen testing, but also in the genetic testing.
Let's say you're twenty years old and we’re not doing a coronary calcium score, what we would use instead to help predict your overall risk would be the blood test, the lipid panel, your other metabolic markers like your haemoglobin A1c, your fasting sugar. And then from the MRI we’d be looking at your body composition, visceral fat deposition, visceral fat level. With MRI we’re now actually able to quantify pretty accurately your visceral fat volume and compare you to other people your same age and gender.
So those things would build into this risk profile, and then the traditional things like how much you drink, how much you smoke, how much sleep you’re getting, if you have signs of sleep apnoea. Even thirty year olds have sleep apnoea now, so those sorts of things all help build a risk profile for young people if you don’t have let’s say a coronary calcium score.
LB: Right and in terms of the genetic analysis, besides being predisposed to familial hypercholesterolaemia or other acute high LDL cholesterol genetics, Q: Is there another set or group of markers that you might be looking at at an early stage that can show someone’s risk?

Polygenic risk scores from my own Health Nucleus genomic report.
Dr Duchicela: What we currently have is a polygenic risk scale that tells you your relative risk. What we do is we look at gene variants that are more present in groups or individuals that have for example coronary artery disease, or who have had heart attacks and then we see if you share those same gene variants, there are weights given to each of these gene variants, and then you come up on a scale of low, medium or high risk.
“I’m really excited what we have in the pipeline with this sort of scoring ... incorporating that with the coronary calcium score and putting it together and getting a global integrated risk score”
But we’re not able to give specific numbers just yet, other than relative risk or absolute risk just because our dataset wasn’t large enough to do that. But what we’re developing right now, you’d essentially get a polygenic risk score or polygenic risk assessment that takes into account these genes associated with familial hypercholesterolaemia, but also other ones that on their own don’t dramatically increase your risk, but in aggregate if you take 20 or 30 of them together they can tilt you one way or the other.
So that’s actually the really exciting part, using polygenic risk scales and scores and building those models out. And we’re just at version one of this I’m really excited what we have in the pipeline with this sort of scoring and also incorporating that with the coronary calcium score and putting it together and getting like a global integrated risk score. So that's where we’re headed, but right now I’d say these polygenic risk scales can tell you you’re a little bit more like people with heart attacks or you’re a little bit less like people with heart attacks but it doesn’t give you an actual number just yet.
LB: That’s really clear and you’ve mentioned version one a few times so it’s clear that one of the things we need to do is get more and more people to come through the Health Nucleus and share their genetic information and family history etc.
One of the things I get really excited about and really enjoy in my visits to the Health Nucleus is going into the MRI machine. I think that’s one of the coolest things you guys do, I love picking the scene, the light color, the music, the things to look at. It’s really awesome.
Q: What kind of data will you be pulling out of the MRI scans and what will you be using it for? Besides the heart analysis and some of the cancer detection, which we already discussed. What will be showing up in that data and what will you use it for?
I’ve split this interview into FOUR parts, due to its length! Part 3 will drop next week!
Previous Post: Part 1
Note: the Health Nucleus has recently appointed a new Medical Director - Dr. Pamila Brar. Dr. Duchicela has transitioned to a role as full-time physician at the Health Nucleus, working directly with patients to optimise their healthcare!
Follow me on Twitter for the latest #Longevity news!
-
RT @rebeccavziegler: The cryonics payoff matrix. Choose wisely my friends. https://t.co/l1rzsmOC2w
-
My rate of aging: 0.79 It’s the new street cred What you got? https://t.co/aHzWHAfCnD https://t.co/L3rZC4QFN2
-
It’s official - I’m co-producing and hosting a new #longevity docuseries, and will begin shooting in a few months… https://t.co/wLGqRrBfbp
-
“The #longevity segment opened my eyes to the groundbreaking advances in biotechnology, health, and wellness. The i… https://t.co/F8YB7PAeMW
-
I’m completely mindblown by what AI has done over the past 3-6 months, and it continues to accelerate… https://t.co/hh0JslucRg
-
Longevity legends take on many shapes and sizes https://t.co/X9vGa7gvOe
I post related #Longevity content to Instagram as well, follow me @nickengerer
FDA & TGA DISCLAIMER
This information is intended for educational purposes only and is not meant to substitute for medical care or to prescribe treatment for any specific health condition. These blog posts are not intended to diagnose, treat, cure or prevent any disease, and only may become actionable through consultation with a medical professional.

Early cancer detection and big data - Health Nucleus interview Part 1

Shaking hands with Dr. Duchicela (left) during my January 2020 visit to the Health Nucleus!
In this post you’ll learn:
Dr. Duchicela’s background
Big Data & healthcare
The definition of ‘Healthy’
Early detection of Cancer
Part 1 - Intro, cancer detection, what is healthy?
In a series of three posts, Longevity Blog interviews Dr. Keegan Duchicela, Medical Director at the Health Nucleus in San Diego, California. Dr. Duchicela received his medical degree from UCSF in 2007. Since the completion of his residency, he has served as the Lead Physician at the Google Wellness Center (Google’s on-campus medical facility), and over the past three years has held several roles at the Health Nucleus including Clinical Director, Medical Director and Physician.
This interview, from the 24 January 2020, walked through a series of pre-written questions with Dr. Duchicela, and is presented in the form of a transcribed audio conversation.
Longevity Blog:
Q: What motivated you to become the medical director at the Health Nucleus? That’s a pretty cool job!
Dr Duchicela:
A: It is pretty cool! My training is in family medicine, so from the get go I have felt there is great value in preventing and detecting disease before it happens and having actual relationships with the patients to really delve into things other than just normal lab values and imaging. I think you really need to get to know the patient, their family, their socioeconomic context, and their culture, as well as where they live to really get a general sense of their health risks, because there are so many other things besides just labs that determine how healthy you are.

Corporate wellness centers, like those run by Premise Health, are becoming more common at big tech companies, like Google. And they recruit top-notch medical practitioners like Dr. Keegan to run them. Source
I come from a different perspective, I didn’t go into medicine to learn about genetics or advanced imaging or even precision medicine, my focus was more on getting to know the person holistically to really enable them to take care of their body, their mind and their family. I looked at health in that context. But as I went through training and through the kinds of places I’ve worked over my career; I worked for a few years at Google helping lead their onsite primary care clinics where I encountered a lot of interesting individuals, engineers who were doing some amazing things with Big Data, I started to really see the value in having a large data set on health metrics and what you can do with that sort of information and the impact you can achieve. I began thinking that the future of medicine for physicians is as good data scientists with excellent bedside manner.
If we could offer this testing at a very inexpensive price point to millions of people, how much better would our health improve overall? I think it could be pretty dramatic to be honest with you.
I really think that’s where we’re heading. And so as a physician I feel like it’s really important to grasp the implications of using Big Data and what it really means and how we can use these analytical tools to predict where we’re going with our health.
after I left Google, I was looking for a company that was doing innovative things
So after I left Google, I was looking for a company that was doing innovative things in this space and really Human Longevity was the only place that I found that’s using imaging, genetics, peripheral blood biomarkers, plus family history and past medical history and putting it all together and getting a comprehensive view of health. So that’s what attracted me to the position. It’s been a wild ride and very interesting to see how the company has evolved and progressed and I think we have a pretty bright future. It’s exciting to be the medical director and that’s kind of how I ended up here.
Looking at this from a primary care perspective, if we could offer this testing at a very inexpensive price point to millions of people, how much better would our health improve overall? I think it could be pretty dramatic to be honest with you.
Longevity Blog (LB): I love that vision and one of the things that attracted me to HLI (Human Longevity Inc.) was one of your founders Peter Diamandis. He’s one of my… ‘heroes’, I’ll call him, a mentor, somebody I look up to. He shapes my thinking a lot and that idea of inexpensive testing for millions and reaching and impacting people positively is a mission that I believe in. The Longevity Blog is me playing my small part in helping to accomplish that.
There’s a really interesting kind of dichotomy that we find between the healthcare industry and the Health Nucleus - and that’s thinking proactively about health care. If I were to go into my doctor’s office, my traditional GP here in Australia and didn’t have any acute symptoms of any sort and told them I was there to optimise my health, they would probably tell me to get outta there because they are there to take care of somebody who’s sick.
Q: So, I was curious what you think the Health Nucleus definition of “healthy” is and how might it be different from a traditional one?
From the Health Nucleus website
Dr Duchicela:
A: I think right now we are in version one of this, in that we are trying to create a suite of testing modalities. We are trying to detect the things that prematurely end people’s lives very early on. The broad categories of these would be things like cancer, metabolic diseases like aneurysm or heart disease, and neurodegenerative disease like alzheimer's. And right now our testing packages or testing suites are set up where we’re looking for those big categories of disease.
When we have enough data and we have enough people go through, and we are able to create advanced risk prediction tool kits and algorithms, that’s when the real promise of a company like this can come to fruition. We do get pretty rigorous metrics from things like genomics and also from the imaging biomarkers like liver fat and visceral fat, but what we really want to do and what we’re currently working on and what really excites me is taking your genomics - let’s say dementia or Alzheimer’s - taking your ApoE status and taking your hippocampal volume metrics from your imaging and also taking into account these other genomic variants that may not contribute to risk in such a large way as for example ApoE does, but on their own could tilt the needle one way or the other and putting this all together with your alcohol consumption, your BMI, your visceral fat levels and everything else and using machine learning and AI to come up with a ten year risk prediction for Alzheimer’s disease.

An example of the brain imagery data collected by MRI at the Health Nucleus, to compute metrics like hippocampal volume. Pictured: my own brain!
That’s where I think the true promise of this testing lies, but those algorithms need to be developed and it really does take a large data set to develop those algorithms. So right now I’d say in terms of our testing modalities we have a really good screening test for these five big categories of disease, but we really want to evolve into becoming the crystal ball for alzheimers, the crystal ball for metabolic disease, the crystal ball for prostate cancer or breast cancer by putting these algorithms or data modalities together and really deriving some good inferences from them, but we need a large data set first. I think that’s the biggest challenge with this.
LB: Right and so that kind of definition of healthy is actually shifting perspective out ahead of time almost, not just are you healthy now, but will you be healthy in the future and what can we do to minimise your risk and hopefully be able to be more predictive with more data and better algorithms that you’re continuing to develop.
Dr Duchicela:
it’s tricky to give a one size fits all definition of health. You really have to take in the context of the individual and see what their values and priorities are and what they want out of their life
A: Yeah and everyone really has their own definition of healthy, because different people have different values. For example I had a patient the other day who is a wine entrepreneur. This is his business, this is how he supports himself and his family, and to tell him, “Hey listen, if you really want to optimise your health and be quote-unquote completely healthy, you may want to avoid the amount of alcohol you’re drinking, because alcohol is a carcinogen.” For him, that would actually negatively impact his lifestyle. He wouldn’t necessarily be living a happy life if he gave up his profession. So, I think it’s tricky to give a one size fits all definition of health. You really have to take in the context of the individual and see what their values and priorities are and what they want out of their life.
And if you ask people about this, it’s not one size fits all. I think that’s the art of this, figuring out what drives them, what motivates them to come in to get assessed; Is it a family member who was recently diagnosed? Is it because they have a grandchild now and they want to be able to be healthy and active for when they get older?

And, at least as a physician that’s what I’m trying to focus on, how do we judge success? I don’t think it’s necessarily just not dying at an early age. It’s essentially living a fulfilling life and accomplishing the goals that you want to accomplish, whether that be having your own wine business and doing that as a profession or living to 100 and being cancer free the entire time. So, I think what we like to do here at the Health Nucleus is focus on the goals of the patient and really try to tailor our recommendations and counseling towards their goals.
LB: That’s great and I love that individual nature of it and the reflection of values and goals that the individual has. You’re right that the definition of healthy has to sit in that spectrum. That’s an encouraging answer and one I definitely agree with.
You just mentioned at the end of your talk there, cancer. Cancer is actually something that has personally impacted me, even directly in my own wife who has had to have two big peritonectomy surgeries for appendix cancer, thankfully she’s in remission now.
I think about the widespread availability of Health Nucleus technologies and MRI scanning etc. and think about if we had had routine access to something like that, how might that outcome have been different.
Q: Now, I don’t want you to go into theoretical outcomes for my specific case, but I’m really interested in helping to share with folks how the Health Nucleus can detect the actual presence of cancer, not just cancer risk but the actual presence of cancer at an early stage.
Dr Duchicela:
A: That’s a great question. When looking at our testing modalities, we have the imaging which is almost like a point-in-time disease test. We’re looking for disease right now, or early early disease, that’s the hope. With the genetic testing, it’s more your disease risk five years, ten years down the road. So the imaging is really powerful in that we can tell you within a few hours after a scan, if there is something concerning, a soft-tissue mass or an aneurysm even.
our goal is to develop a test that doesn’t use radiation, that we can give safely to many many people, that covers most cancers and then have a suite of tests to fill in the gaps essentially.
With our imaging, that’s really the goal, we cover some cancers pretty well, but we also have some gaps in our cancer coverage, just to be completely transparent. We don’t pick up colon cancer or certain other GI cancers very well, the MRI results are limited because we don’t have people do a bowel prep ahead of time, so we would still recommend a colonoscopy or a Cologuard test for that.
Certain pulmonary cancers you can’t get too well just yet with MRI but we’re working on that. No screening test is perfect, and you can’t catch every cancer with one single test, but our goal is to develop a test that doesn’t use radiation, that we can give safely to many many people, that covers most cancers and then have a suite of tests to fill in the gaps essentially.

My own Health Nucleus MRI scan (pictured), from 2018.
Or maybe they can go through their traditional medical provider to do the colon cancer screening if we don’t have a good option for it here. So in terms of developing a test for cancer, it’s tricky because we don’t want to say that if you have a completely clear scan you’re cancer free, there are gaps and limitations with the current technology. But over time as we are able to get more patients through, we’re able to do better processing on the images, so hopefully we will start to fill in those gaps with better early detection of cancer.
LB:
Q: You’ve made very clear caveats on the limitations there, but where does your technology excel and succeed? There would definitely be some anecdotal examples of detecting certain types of cancer at an early stage. You certainly have some excellent technology in that space, could you elaborate a bit further on that?
Dr Duchicela:
I think where it excels is that we’re able to get really good images without having to use contrast and that’s really important if we’re trying to scale this and bring it to many people at a low price point, we want to make it safe too. We do have pretty good post processing.
Let’s take prostate cancer for example, most men will die with prostate cancer, rather than from prostate cancer. So the trick is, how do we know which prostate cancer is going to be an issue and is going to prematurely end your life and which is so slow growing that they will most likely pass away from other things instead of the prostate cancer. With the post processing that the computer scientists and radiologists, people much smarter than myself, have developed, they’re able to light up and differentiate with the software these higher grade lesions in the prostate that have a higher chance of being a concern and being more aggressive and truly cancerous.

Image Credit: UC London. Prostate cancer screening by MRI is becoming more widely accepted. That’s very good news for early detection and treatment. Source
So that kind of differentiation on the back end is really powerful. We don’t want to be detecting things that won’t really harm someone in the long run. If you’re familiar with prostate cancer screening in general, it’s pretty controversial just because if we find something, we are almost obligated to biopsy it and there can be complications with biopsy. So we really want to make sure that we are finding things that are meaningful, and I think with the post processing that we do with our scans we can make that differentiation and better guide them to say alright this a lesion that is at a much higher risk, so we would suggest you get a biopsy, as opposed to alright this is lower risk lesion based on our scans and it may be more reasonable to watch and wait, get a serial PSA, that sort of thing.
LB: That makes a lot of sense, and you’re right in terms of wanting to minimise false detection or follow up treatment or biopsy to the really significant or possibly progressive forms of the cancer. That’s really fascinating.
We’ve talked a little bit about cancer, another big killer and one that is kind of a function of how old you are and how long you’ve been alive and a number of genetic risk factors is actually cardiovascular disease and in particular atherosclerosis.
I understand my risk as a man in his thirties is low for an acute event now, but that it’s really decade on decade buildup of plaque and inflammation and wear and tear on the arteries that increases the risk…
Q: So how does coming to the Health Nucleus help inform someone about their risk as they get older and what they can do as a young person to minimise the risk of atherosclerosis and cardiovascular disease?
I’ve split this interview into four parts, due to its length! Part 2 is coming soon :)
Note: the Health Nucleus has recently appointed a new Medical Director - Dr. Pamila Brar. Dr. Duchicela has transitioned to a role as full-time physician at the Health Nucleus, working directly with patients to optimise their healthcare!
Follow us on Twitter for the latest #Longevity news!
-
 RT @nickengerer: Join a team, do a sport. Staying fit is easier with a clear purpose Bonus: you just might live longer Pic: Byro… https://t.co/L5yHxHJXas
RT @nickengerer: Join a team, do a sport. Staying fit is easier with a clear purpose Bonus: you just might live longer Pic: Byro… https://t.co/L5yHxHJXas -
Calcium AKG Alpha Keto Glutarate Supplement Review https://t.co/K7keDM3Lyn
-
Mitopure Review - Does this Urolithin A supplement actually work? https://t.co/0Y6Bx4yA7h
-
How Fast are You Aging? A Biological Age Test for Rate of Ageing with Ryan Smith of Trudiagnostic (Part 2) https://t.co/5SZW3Or6JJ
-
What is the Most Accurate Biological Age Test? An Interview with Ryan Smith of Trudiagnostic (Part 1) https://t.co/wdIxtTVeq0
-
One Skin Review - Self-Experiment Before and After Results with OS-01 https://t.co/3hqzLtfVa3

Boosting the immune system with IV therapy - Does it help?
Amidst a global COVID-19 Crisis, immunity is on our mind
In this post I’ll cover:

The basics of IV therapy
An experiment I ran with an immune boosting IV therapy
White blood cell blood tests
Review of the data I collected
Making the best conclusion we can on the value of IV therapy based on the data collected
It just so happens, I recently ran an experiment with immune IV therapy to answer - is an immune boosting IV treatment worth it?
A quick video sharing the experience of getting an IV therapy at NextHealth in West Hollywood
Most of us have had an IV in our lifetime. They are exceptionally helpful for delivering hydration and electrolytes to patients in-hospital. IV stands for ‘intravenous’, as they function via the insertion of a sterile catheter into the vein (most commonly in the arm or wrist). Sometimes, in addition to hydration, they are used as a method of ‘infusion therapy’ where, for example, medication is delivered intravenously.
Traditionally, IVs were only delivered in hospitals, but then after a time, shifted to outpatient clinics, and now are populating health & wellness centres around the world. Chances are, if you Google for an “IV clinic" in the US, Australia or Europe - you’ll find one near you! In each instance, a trained nurse is the most likely the person who will insert the catheter and set-up the infusion treatment.
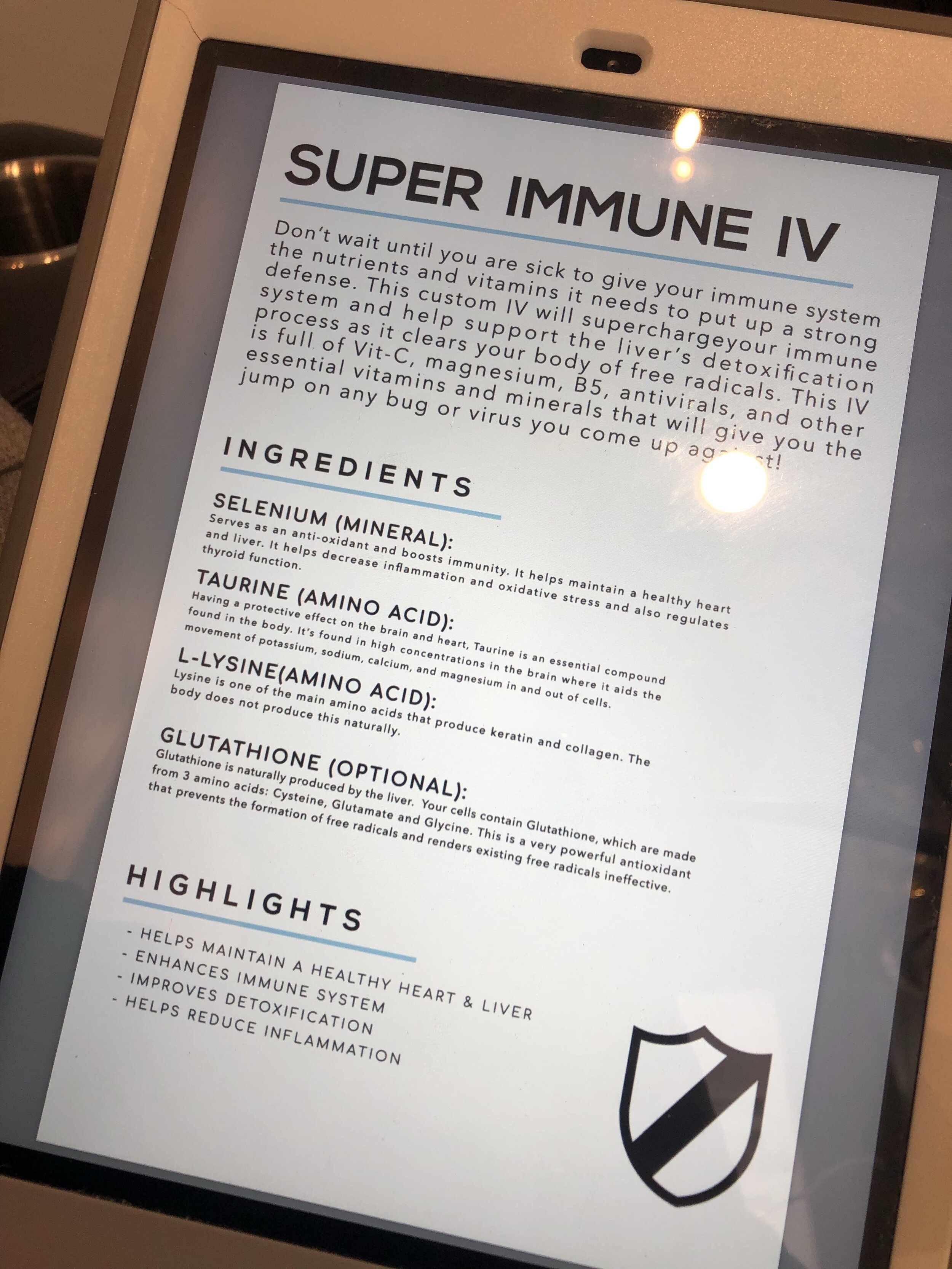
IV therapy at NextHealth - Super immune
I recently undertook my first ever IV therapy (outside of a hospital) at NextHealth in West Hollywood, Los Angeles. After undergoing a micronutrient test to inform my selection of treatment, I settled on trying out the Super Immune IV therapy. My motivation for this was that on my previous long-haul roundtrip from Sydney to Los Angeles, I became quite ill upon return. So this IV therapy caught my interest during a following roundtrip Sydney-LA about 2 months later.
Super immune IV - the claim
The Super Immune IV claims to ‘supercharge’ the immune system with Vitamin C, Magnesium and Vitamin B5 plus Selenium, Taurine, and L-lysine. I took a photo of the information NextHealth provided to me on the contents & benefits of the treatment.
Forming a hypothesis: Immune IV Therapy - Does it work?
Now, being the biohacker enthusiast I am, I naturally decided to undertake an experiment in order to try to measure the impact the Super Immune IV therapy had on my immune system. With any good experiment, we must form a hypothesis, design a framework for testing it, collect relevant data, analyse these data and form a conclusion. So let’s start with - what was the hypothesis?
Hypothesis: the Super Immune IV will measurably boost my immune system and keep me from getting sick during my international travel
The Experiment: Two long haul roundtrip flights from Sydney to Los Angeles
As I mentioned above, I completed two long-haul, roundtrip flights from Sydney to LA. Both lasting 7-8 days. The first was in November 2019 (Trip #1) and the second was in January 2020 (Trip #2). During both trips, within 4 days of the first flight, I completed a comprehensive panel of blood tests (one at NextHealth, one at the Health Nucleus). Trip #1 had no Immune IV. Trip #2 had an Immune IV therapy on Day 2 of the trip (3 days prior to the trip’s blood test).
There are many factors that could influence the results of this experiment, but as with nearly every biohacker experiment this is always the case. In fact, it is a fundamental limitation of running self-experiments that they cannot be perfectly controlled due to the sheer complexity of our biology and its interaction with our environment. This doesn’t mean one should not do their best to provide a controlled environment! It just means we need to mindfully interpret the results of the experiment.
However, I took a number of measures to provide the best control possible. Diet was unchanged. Sleep was very similar on both trips, with ~7 hours of relatively poor sleep on the flight over (according to sleep tracking data). I also employed the same jet lag adjustment strategy that I have developed on both trips. Neither had more than 1 glass of alcohol (wine) intake within 2 days of the blood tests. Both had moderate levels of exercise (plenty of walking, some light running).





Caption: Step 1: Chill in sweet chairs. Step 2: Get your arm warmed up. Step 3: Get skilfully stuck. Step 4: Pump in the goodness! Step 5: Relax! (It takes about 30 minutes)
Understanding the data points
For the layperson, there is a need for us to first dive into what the data I plan to share represents. The same data was collected for both Trip #1 and Trip #2.
White blood cell count (WBC)
White blood cell count (WBC) represents the total number of leukocytes in a volume of blood. Leukocyte is just fancier way of saying white blood cell, which are the cells of the immune system that protect us from infectious disease and foreign material (e.g. toxins, allergens).
If WBC count falls below the standard reference range of 4k/uL, this signals that the supply of white blood cells has been depleted. This is most commonly caused by an infection, but can also be the result of chemotherapy or radiation treatment (hence why many cancer patients have compromised immunity). If you are noticeably fighting a viral or bacterial infection, it is likely your WBC will fall below this value, before rebounding as your immune system ramps up.
A selection of white blood cell types. Source: unknown
White blood cell differential
Whereas the WBC represents the total number of white blood cells present per unit of blood, the differential blood count provides a breakdown of each type of white blood cell. This is most commonly used in medicine to search for any abnormalities in the overall populations. Differentials can be useful in the diagnosis of infectious disease, allergic reactions and during monitoring for adverse impacts from certain drugs (e.g. cytotoxic ones used in the treatment of cancer).
There are many excellent sources of information on the ‘basics’, and in my background research I found Medscape to be a particularly useful source.
Neutrophils - the most common type. Neutrophils function by travelling to the site of an infection to release enzymes to ward off viruses or bacteria which are invading the body
Lymphocytes. These search and destroy machines breakdown into two types:
B-cells fight exogenous (those coming from outside the body) bacteria, viruses or toxins.
T-cells target the body’s native cells in the case that they become infected by a virus or those that become cancerous.
Monocytes remove foreign material, remove dead cells, and boost the body's immune response.
Eosinophils fight infection, inflammation, and allergic reactions. They also defend the body against parasites and bacteria.
Basophils release enzymes to help control allergic reactions and asthma attacks.
This is a heap of new information for most us, so here are few key take-aways for understanding the upcoming results and discussion:
A fall in WBC below the reference range of 4k/uL is:
indicative of an infection (in my case on Trip #1, a respiratory virus)
most often due to depletion of the neutrophils who are ravelling to the site of an infection as first responders
The standard reference range expects neutrophil count to be greater than 1.5x10E6/uL; for me, a value of ~2.4x10E6/uL is baseline.
Interpreting the results
In addition to the two WBC and differentials tests I had performed in November 2019 (Trip #1) and January 2020 (Trip #2), I have also included data from May and August 2018, to provide baseline measurements. During both of these baseline measurements I was healthy and without an immune system compromise.
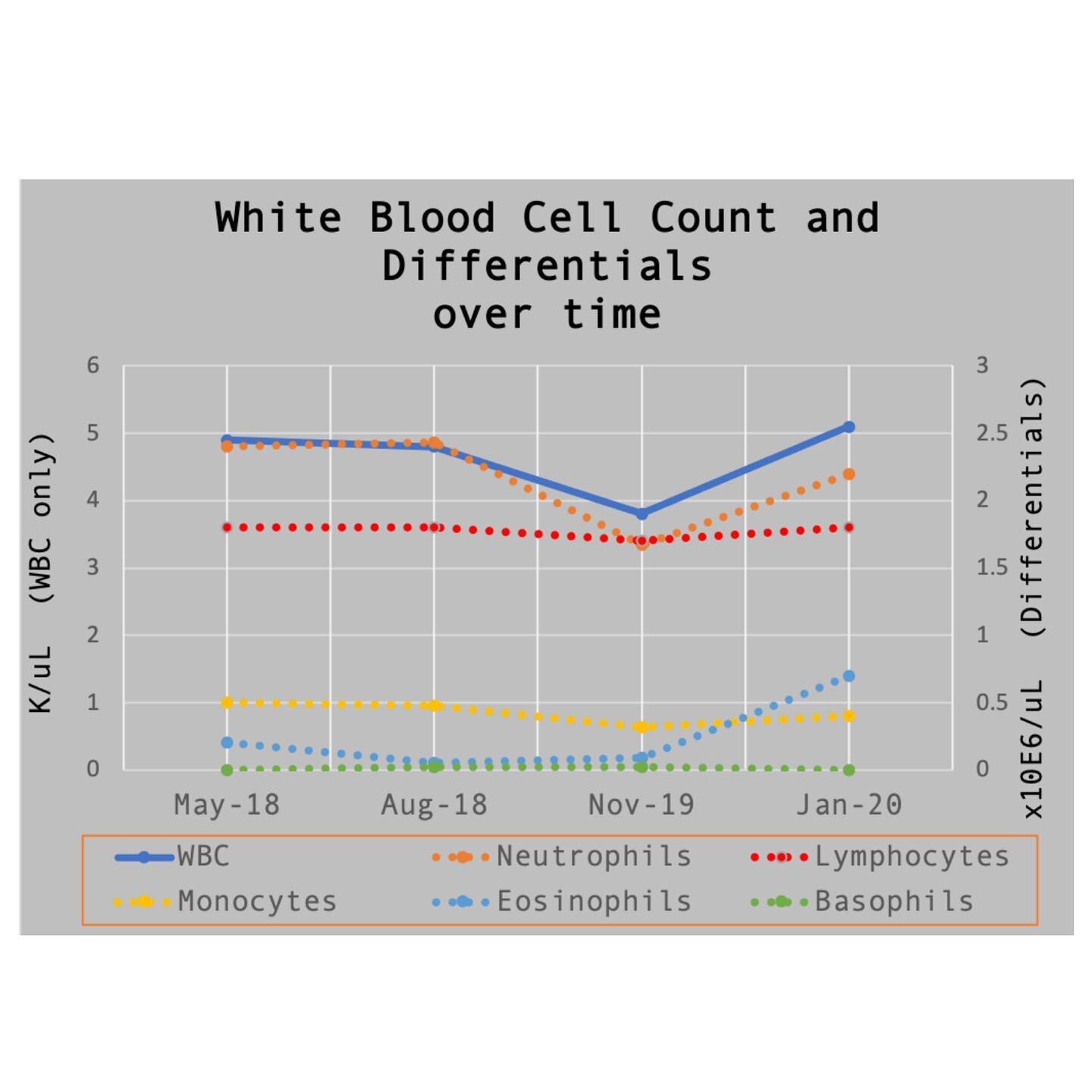
White Blood Cell Count (left-hand axis) and White Blood Cell Differential (right-hand-axis) over four blood tests. Trip #1 data is “Nov-19”, where I became unwell. Trip #2 data is “Jan-20” where I received the Super Immune IV therapy at NextHealth.
From the provided chart, a few observations can be drawn
Baseline values for WBC and differentials are steady (May-18, August-18), evidence of a good set of control data
There is a clear drop in WBC, Neutrophil and Monocytes in Nov-19 (Trip #1)
Trip #1 WBC values fall below the reference range values, indicative of the viral infection
Trip #2 Neutrophil values are about 15% below baseline
Trip #2 WBC, Lymphocyte, Basophil values are in-line with the baseline values
Trip #2 Eosinophils are 3.5-4x baseline value
Interpreting these results is complex, but given my unique perspective as the experimenter, I offer the following supplementary information and observations.
WBC which is indicative of the overall immune system’s robustness are higher during Trip #2 than in Trip #1
Neutrophil count during Trip #2 is not in-line with baseline, suggesting it is possible that my immune system was being challenged, but not overcome (as is expected during international travel)
The increase in Eosinophil (Eos) count in Trip #2 is probably best explained by my legs being covered in angry red scrapes from a trail run where I got lost and had to scramble through bracken fern two days prior to my drip (ouch!). Recall from the above these white blood cells fight inflammation and allergens (those angry red scrapes!).
Point #3 suggest that there would be a downward revision of WBC to approximately 4.7k/uL for the purposes of comparing it to baseline and Trip #1 (adjusting WBC to not have the cofounding signal from the Eos elevation). This still leaves the WBC similar to the baseline values of 4.9 and 4.8 k/uL.
Discussion: Does the data support getting an Immune IV treatment?
So, let us return to the hypothesis - that my intake of an IV immune therapy would measurably improve my immune system during my long-haul flight and international travel and I would not get sick.
We so far have discussed one primary source of data and analysed it in this context. Overall, based on my ranges of 'normal' from my historical blood tests, the results after my NextHealth Immune IV, and Trip #1 where I became ill from the travel, it does appear there was a measurable improvement in my immune function on Trip #2.

While not perfect, I choose to wear a facemask whenever I travel through airports. These are not guaranteed to provide effective protection from contagious disease, and are advised against by some medical experts. It is my personal opinion that they do provide some measure of protection when compared to not wearing one.
However, this it is difficult to make the conclusion that the Immune IV kept me from getting sick with high confidence. I could have simply picked up a particularly nasty virus on the way to/from LA on Trip #1 and not on Trip #2. In this scenario, the Immune IV treatment could arguably have little to do with the outcome or any of the apparently measurable difference between the two.
Instead, I offer that it is more valuable to draw a different category of conclusion on the subject of whether the Super Immune IV is worth it. To do so, we need to return to both (a) the fundamentals of international travel, (b) the outcome I desired (to not get sick) and (c) the value of the outcome versus the cost.
With respect to (a), it is known that getting poor sleep, experiencing timezone changes, and being exposed to numerous pathogens (in the airport, in the airplane) undoubtedly challenges the immune system. It is commonly accepted that one should take action to protect themselves when travelling for these reasons.
Secondly, and in my view, more importantly, (b) - I did not get sick on Trip #2, which is the outcome I desired. Becoming ill on return after Trip #1 was miserable, cost me time at work, and put my family and friends at risk of contracting the pathogen I was carrying.
The overall conclusion: Immune IV therapy is worth it (for me)
Given the experiment, data and resulting discussion, I offer the following conclusions:
1) It is completely possible and perhaps probable the Immune IV therapy boosted my immune system and kept me from getting sick on Trip #2
2) Getting an immune IV therapy is an appropriate risk management, strategy for international travel
This latter conclusion is based on the principles of risk management, where one weighs the nastiness of the outcome against the cost of managing the risk. In this context (c), I’d argue the IV treatment to be well worth it at $189USD.
As an outcome from this experiment, my personal choice will be to continue to drop into NextHealth on my long-haul trips to the United States and get that IV goodness dripped into my vein! If you’re a travelling businessperson with similar level of resources (IV treatments are relatively affordable to you) and level of risk (becoming unwell is quite costly), you would likely also benefit from partaking in immune boosting IV therapies.
I’ll be sure to collect additional WBC and differentials data on my next trip to the US and post a follow-up blog to accompany this one. Be sure to subscribe to be notified when I do!

-
RT @rebeccavziegler: The cryonics payoff matrix. Choose wisely my friends. https://t.co/l1rzsmOC2w
-
My rate of aging: 0.79 It’s the new street cred What you got? https://t.co/aHzWHAfCnD https://t.co/L3rZC4QFN2
-
It’s official - I’m co-producing and hosting a new #longevity docuseries, and will begin shooting in a few months… https://t.co/wLGqRrBfbp
-
“The #longevity segment opened my eyes to the groundbreaking advances in biotechnology, health, and wellness. The i… https://t.co/F8YB7PAeMW
-
I’m completely mindblown by what AI has done over the past 3-6 months, and it continues to accelerate… https://t.co/hh0JslucRg
-
Longevity legends take on many shapes and sizes https://t.co/X9vGa7gvOe
-
RT @BradStanfieldMD: Avoid These Popular Supplements (shout out to Professor Matt Kaeberlein @mkaeberlein & Professor Brian Kennedy… https://t.co/cy9CXldgUS
-
Who are influential persons in #longevity who are of Asian, African American or other “minority” group in the US?
-
The AI powered future is here 🦾 Contrary to the narrative, you’re not going to be replaced in the workplace by AI… https://t.co/BojTzyfDzA
-
I built and exited my first company today A big moment in my entrepreneur journey What’s next? All in on… https://t.co/5oTo3IjSyN

Four tools for managing cardiovascular disease risk
Cardiovascular Disease kills But longevity technologies help manage risk
In this post, we present you with four immediately actionable ways to ASSESS your risk
If you’re like us — you’re excited about the imminent increases to our healthspan that longevity technologies will soon offer us. However, if you want to stick around long enough to take advantage of all of the soon-to-be available lifespan and healthspan boosting technologies, you need to make sure you don’t die in the process!
But how will you die? Probability states it will be one of the four deadly killers
Atherosclerotic coronary heart disease is the single leading cause of death of men and women in the United States [Source: Medscape]
Ever since science effectively cured infectious disease through antibiotics, vaccinations and the like, there has been a distinct shift in what kills humans to the four deadly killers, which are considered ‘age related diseases’.
These are — cardiovascular disease, neurodegenerative disease, metabolic disease and cancer. If you manage to escape the most likely causes of death as a young person, which are largely accidental death (mostly car accidents), homicide or mental illness related (suicide) — then it is most likely that one of those four deadly killers will end your life.
But here’s the good news — there’s a growing body of immediately actionable longevity technologies that you can engage with to offset your risk of dying of these diseases.
In a series of posts on the topic, we’ll cover a few key resources at your disposal for managing your risk for each of these four categories.
First-up, cardiovascular disease.
Deadly Killer #1 — Cardiovascular disease
Heart attack, stroke, thrombosis, heart failure — the chances are overwhelming that you have lost someone important to you in your life to one of these causes.
It is often seemingly sudden, but in most cases, the acute cause of death by cardiovascular disease has been brewing for a very long time — decades even.
From A to D, the progression of atherosclerosis. At A: healthy aorta with no disease. D: an abundance of plaques and ulcerations.
The term ‘cardiovascular’ encompasses disease of both the heart and blood vessels, which is driven by the build up and eventual displacement of plaque that accumulated in the arterial wall in a process called ‘atherosclerosis’.
It’s not our role to explain all of the mechanisms of this disease.
Instead, we’ll focus on four actionable tools you can work with your doctor to obtain access to, which will help you assess your risk profile and detect any elevated risk of an acute event (e.g. heart attack, stroke) at an early, treatable stage:
1. Action 1 - Test your ApoB (“A-PO-B”)
Stop using your LDL-C as your only risk assessment tool (The “LDL” value too commonly called the “bad” cholesterol), and add tracking of your ApoB.
ApoB is a particular type of molecule attached to the types of lipoproteins carried by your LDL (and VLDL) that are the most likely to enter the arterial wall and lead to plaque formation.
You need to know *how many* of these atherogenic particles you have present in a given volume of you blood — this drives your risk.
Your ApoB value is influenced by diet and lifestyle and can be controlled with pharmaceutical intervention and possibly through certain forms of supplementation.
Learn more about ApoB at Healthline.
Self-order your own Apo-B test (+other cardiovascular markers)!
No doctor required!
HealthLabs.com (USA) - Single Test
UltaWellness (USA) - Panel
I-Screen (Australia) - Panel
2. Action 2 - Do you have elevated Lpa (”L-P-little-A”)?
Lpa is another cardiovascular disease bad guy that may be in your bloodstream.
Lipoprotein-a is a particle which carries cholesterol, fats and proteins and is made by your body, and how much of it you make is inherited.
Elevated levels of Lpa increase your risk of a heart attack or stroke as they are known to cause atherosclerosis.
You certainly need to know if you carry the genetic risk factor, and the earlier the better (i.e. get this test done as early as possible)!
Levels of Lpa don’t change much over one’s lifetime, so testing it once is enough in most cases!
Know your Lpa status, and better know your risk, and whether or not you should modify your diet, lifestyle and treatment options.
Learn more about Lpa from the lipoprotein-a foundation
Self-order your own Lp(a) Test
No doctor required!
HealthLabs (USA) - single test
UltaWellness (USA) - Panel (includes ApoB)
i-Screen (Australia) - Panel (includes ApoB)
3. Know your Coronary Artery Calcium scan score
Coronary artery calcium (CAC) scans are created by using computed tomography (CT) scans, which are a type of X-ray scan, to detect the presence and quantity of coronary artery calcification (the warning signs of atherosclerosis).
A CAC test reveals both the location and quantity of calcium located in three of the main coronary arteries. The scan provides a score which represents your risk.
The lower the better! This score will change over time, and is known to increase with age, so it is important to record it regularly (in a manner that balances the downsides of the X-ray radiation — ask your doctor what’s best for you).
Atherosclerosis is a disease of ageing, and that means your risk is increasing over time. If you are aged 50 or above and have never had one — work with your doctor to get one performed.

Read more about CAC scores in our interview with Health Nucleus Medical Director Keegan Duchicela.
4. Track your inflammation with C-Reactive Protein (CRP)
At its roots, atherosclerosis is known to be intimately connected with inflammation.
In fact, it is often damage to the arterial wall that attracts the formation of plaque in the first place.
This damage occurs over time, and is known to be increasingly likely with high blood pressure and high blood glucose levels.
CRP is a very common and relatively low cost blood test that can be easily ordered up by your doctor, and should be tested annually at the very least.
High levels of CRP are indicative of increased risk of cardiovascular disease, and once again can be influenced by changes in diet and exercise.
If you have the option, go for the high-sensitivity CRP (hsCRP) test if possible!
Self-order your own hsCRP Test
No doctor required!
HealthLabs (USA) - single test
UltaWellness (USA) - Panel (includes ApoB & Lpa )
i-Screen (Australia) - Panel (includes ApoB & Lpa)
Take Action!
Everything that we have discussed in this post encompasses longevity technologies that are available to you NOW.
Ultimately, it is up to YOU to demand access to these technologies, in one way or another. No one is going to do that for you.
If you are aged 50 or older, the importance of getting each of these tests performed is exponentially more important with each decade of life!
Follow us on Twitter for the latest! @longevity_blog
-
RT @nickengerer: Join a team, do a sport. Staying fit is easier with a clear purpose Bonus: you just might live longer Pic: Byro… https://t.co/L5yHxHJXas
-
Calcium AKG Alpha Keto Glutarate Supplement Review https://t.co/K7keDM3Lyn
-
Mitopure Review - Does this Urolithin A supplement actually work? https://t.co/0Y6Bx4yA7h
-
How Fast are You Aging? A Biological Age Test for Rate of Ageing with Ryan Smith of Trudiagnostic (Part 2) https://t.co/5SZW3Or6JJ
-
What is the Most Accurate Biological Age Test? An Interview with Ryan Smith of Trudiagnostic (Part 1) https://t.co/wdIxtTVeq0
-
One Skin Review - Self-Experiment Before and After Results with OS-01 https://t.co/3hqzLtfVa3
-
Regrowing Knee Cartilage and Restoring Joint Health Naturally. An Interview with Reviiv Light CEO Forrest Smith - P… https://t.co/O671LROvzw
-
RT @nickengerer: 90 years old, what to do? A half Ironman, why not? Hiromu Inada now holds the record for the oldest ever competi… https://t.co/wv7NPhslUM
-
One Skin Before and After - Skin Aging in the Future: An interview with OneSkin CEO Dr Carolina Reis - Part 2 https://t.co/RlLlqRurT6
-
RT @Do_Not_Age: Our new ingredient, Spermidine, reduces amyloid plaques and inflammation of the brain in rodents Check our Science… https://t.co/RgehOqmVtf
FDA DISCLAIMER
This information is intended for educational purposes only and is not meant to substitute for medical care or to prescribe treatment for any specific health condition. These products are not intended to diagnose, treat, cure or prevent any disease.

Assessing the aesthetic age with advanced facial scanning technology
How old you ‘look’ is about far more than vanity
In my last post, I shared three online tools for assessing your biological age. In this follow-up post, I want to discuss another segment of technologies, related to assessing one’s apparent youthfulness. This refers to how old one ‘looks’. In my last post on this topic, I coined the term aesthetic age, so let’s roll with it.
How old you look has MUCH more to it than simple vanity. I know from personal experience that many people who utilise available technologies to look younger often will keep their efforts to do so relatively secretive, in order to avoid the negative stigma that has become attached to it. “Oh, she’s definitely had work done”, is a typical example that highlights the stigma I refer to.
But your apparent youthfulness is an professional asset, and does wonders for your subjective experience through boosted confidence and increased self-image. You need do nothing more than ask someone in your life who bears the marks of old age in their face to describe their experience venturing out into the world on a day to day basis. Many of them will tell you they ‘feel invisible’, receive poorer levels of service in the retail and restaurant industry, and miss the days of being attractive to members of the opposite (or same!) sex.
Beauty that is skin deep
There are many factors that regulate of one’s aesthetic age, and it can be difficult to find an objective measure of how old one looks. I previously shared how I like to turn the question ‘how old are you’ into a game of ‘well, how old do I look?’, getting a median guess of ~27 years old. This is one useful way of forming a statistical approach to the question, as in my experience the results form a relatively neat gaussian distribution.
But as a scientist, I crave something more data driven - and that’s what inspired my latest visit to NextHealth in West Hollywood. Last November during my first visit to NextHealth I learned about an incredible piece of technology for assessing your aesthetic age - the Visia. This unit utilises multispectral (including UV spectrum) imagery to look deep into the skin of your face for clues about its health. To complete the scan, you place your chin and forehead into the unit, and hold still while a series of 3 flash photography images are taken, and submitted to the Skin Analysis System’s algorithms. But let’s let the expert (Matthew at NextHealth) explain it…
The scan took only a few seconds, here is what it looked like
How old is my face?
Visia scan results through eight different actionable categories
The results came quickly, and thankfully, pegged me a bit under my actual age (34) with an aesthetic age of 31. This is much older than my biological age of 22 years old, so while it is a relatively youthful result - I’d like to know how I can do better! (If you’re interested, you can listen to Matthew describe my results here)
This is one of the things I LOVE about NextHealth. They, like me, are obsessed with optimising human performance. In the 30 minutes following my scan, Matthew diligently and patiently answered my many questions about how I can work to improve the apparent youthfulness of my skin.
Here are two areas of action I will be experimenting with improve my aesthetic age before my next Visia scan.
UV damage
I live in Australia, where the sun’s ultraviolet rays are known to be extra intense (thanks Ozone hole!), and the relative rates of skin cancer are roughly double most other areas of the world. In fact, roughly 2 in 3 people will get some form of skin cancer by the age 70. I’d very much like to be in the 1/3 that doesn’t!
The Visia scanner was able to highlight the need for me to take much more care with my facial sunscreen routine, and search out proactive solutions for reducing my UV spots. One great option is the Broadband Light (BBL) lasering, which focuses an intense beam of light energy into the skin of the face can destroy these spots and quite literally reverse the age of your skin.
I’m definitely going to be trying this out in the near future! And of course, I’ll share the experience with you :)
Wrinkles
Wrinkles in the skin can be addressed in several ways, but I’m relatively uninterested in the ones that cannot lead to a lasting difference (e.g. creams that plump your skin or wrinkle-fillers or makeup, etc). So far, there are two options that I am experimenting with:
1) Retinol
Before (Left) and After (+ 6 weeks at 2% retinol daily)
Prior to the Visia scan, I had actually run a 6 week retinol experiment on the skin surrounding my eyes. Maybe that has already led to me appearing younger than my 34 years, given I look 31!
By applying a 2% retinol (which is actually just the active form of Vitamin A), I accelerated the turnover of the cells on the top layer of my skin, bringing a more youthful layer to the surface. I found it difficult to capture the difference meaningfully on my iPhone camera, but I did take some before & after photos. IRL (that’s “In Real Life” for the less hip crowd) the results were quite obvious. My ‘crow’s feet’ had receded, and the skin around my eyes was visibly less wrinkled. I plan to continue my use of retinol, increasing the concentration of the serum to at least 4%.
2) Botox
If you’re like me, you are likely very skeptical of the benefits of botox injections. I was under the impression that they were merely a temporary fix, would leave your face expressionless and that botox will make your wrinkles worse if you stop the injections.
Upon further research and consultation, I found none of these things are actually true. But what is important to note is that there are a variety of factors that go into a successful treatment regimine that will actually have a meaningful impact on your aesthetic age.
First - while botox might help you look more youthful in the short-run, it really should be viewed as a way of ‘maintaining aesthetic age’ rather than turning back the clock. Creases and wrinkles in your face are slowly deepened over time by long-term repetitive use (think of folding a piece of leather over and over and over…). Botox fill reduces this repetitive strain on your skin.
Second - botox injections are more of an ‘art’ than a strict science. Seeking out someone who is experienced, can demonstrate skilled results through testimonials and has an absence of bad reviews to their name is a must.
Third - consistency is key. It takes awhile to work out the right strategy for achieving the results you’re after, and if you’re not willing to put up the budget to keep the practice up for the long-haul, you might be better off not trying this one at all.
I’m currently in the research phase with the botox option on my end, so stay tuned and I’ll be sure to share any self-experimentation I undertake with botox.
How can you access this technology?
My first Visia scan and consultation with NextHeath were complimentary - so if you live in LA or have any travel plans through the area, your first choice is obvious!
However if you’re not in LA, it is very likely that you can find a local aesthetic care facility that has a Visia unit, as they are relatively popular. I am currently writing to you from San Antonio, and a quick internet search revealed at least two options. I even tested the capital cities of Australia and found locations there as well. A simple Google of “Visia scan near me” seems to be a handy approach. The Canfield Science (Visia’s manufacturer) website lists distributors in North America, Central America, South America, Europe, Middle East, Asia, Oceania and even Africa!
-
RT @rebeccavziegler: The cryonics payoff matrix. Choose wisely my friends. https://t.co/l1rzsmOC2w
-
My rate of aging: 0.79 It’s the new street cred What you got? https://t.co/aHzWHAfCnD https://t.co/L3rZC4QFN2
-
It’s official - I’m co-producing and hosting a new #longevity docuseries, and will begin shooting in a few months… https://t.co/wLGqRrBfbp
-
“The #longevity segment opened my eyes to the groundbreaking advances in biotechnology, health, and wellness. The i… https://t.co/F8YB7PAeMW
-
I’m completely mindblown by what AI has done over the past 3-6 months, and it continues to accelerate… https://t.co/hh0JslucRg
-
Longevity legends take on many shapes and sizes https://t.co/X9vGa7gvOe
-
RT @BradStanfieldMD: Avoid These Popular Supplements (shout out to Professor Matt Kaeberlein @mkaeberlein & Professor Brian Kennedy… https://t.co/cy9CXldgUS
-
Who are influential persons in #longevity who are of Asian, African American or other “minority” group in the US?
-
The AI powered future is here 🦾 Contrary to the narrative, you’re not going to be replaced in the workplace by AI… https://t.co/BojTzyfDzA
-
I built and exited my first company today A big moment in my entrepreneur journey What’s next? All in on… https://t.co/5oTo3IjSyN
What's My Age Again? Quantifying Biological Age with Three Free Online Tools
“How old are you?”
It’s a common question, and one that we often use in early conversation with acquaintances of all sorts. I’ve noticed just how common a query it is, because I’ve turned it into a fun guessing game, where I reply - “Well, how old do you think I am?”. People will often take a few moments to look at my face, and spurt out their guess without much hesitation. I’ve been casually keeping track of the responses, and the median age is currently 27 (range 24 - 30, 15 responses) - not bad for a 34 year old.
This fun little guessing game starts to beg a deeper, biological question. The difference between how old we look (we might call this one’s aesthetic age) versus our actual chronological age, varies from person to person. Looking at my classmates from high school or college over the years has been quite remarkable in this regard - many of my male classmates are now balding or have grey hair, others seem to have many wrinkles or sagging facial features already, many are overweight or obese - but a select few are trim, fit, glowing and youthful in appearance. So onto that biological question - are there measurable differences between people of the same chronological age that may shed some light on the seemingly different rates of aging I observe across my peers?
For a great, layperson explanation of the epigenetic ageing process, and what to do about it - Grab yourself a copy of “Lifespan” by Dr. David Sinclair

Well, fairly recently, the answer to this question has become a very clear yes. Enter the concept of biological age - where measuring representative variables in human biology have yielded remarkably accurate answers to this tricky question. There are several methods of approach, but by far the most widely discussed and accepted in the scientists exploring this topic are methylation clocks, which track changes in methyl groups in the epigenome. The epigenome is the system that controls how our genome is expressed, and this is known to change as we age. Later this year, I have plans to test and review several different biological age tests, including methylation clocks and other tools for tracking the epigenome and telomere length.
Given this emerging field of science, and new technologies that are following it, I have spent much of my recent longevity research efforts exploring the tools that are available to biohackers and wellness enthusiasts like myself for quantifying biological age. Today, I’ll share three different online tools that you can leverage, and share my results with you.
Biological Age Tool #1 - Phenotypic Age
[EDIT: Alternative direct download for spreadsheet hosted at the above link]
“Phenotypic Age” was first discussed in two separate studies, which you can find here (study 1 and study 2 -< note that Steve Horvath is one of the authors, who has pioneered the methylation clock work mentioned above). Phenotypic Age is calculated based on 9 biomarkers and measured chronological age using a cohort of 11,432 adults (a range of 20-84 years old). I was first introduced to this tool by Dr. Michael Lustgarten, who also blogs on longevity related topics, and was recently able to test out this tool for myself, thanks to the 15 vials of blood I gave at NextHealth.
Using the results from my Total Baseline test, and the excel spreadsheet located here (EDIT: some readers have reported the spreadsheet link is not working, so here is an alternative direct download) , I was able to enter the following information to reveal my phenotypic age. This includes information about the shape and size of my red and white blood cells, inflammation (C-reactive protein), albumin (protein in blood plasma) and creatinine (a byproduct of muscles and measure of kidney performance).
My biological age: 22 years old. That’s 12 years younger than my chronological age of 34! Hey - I must be doing something right :)
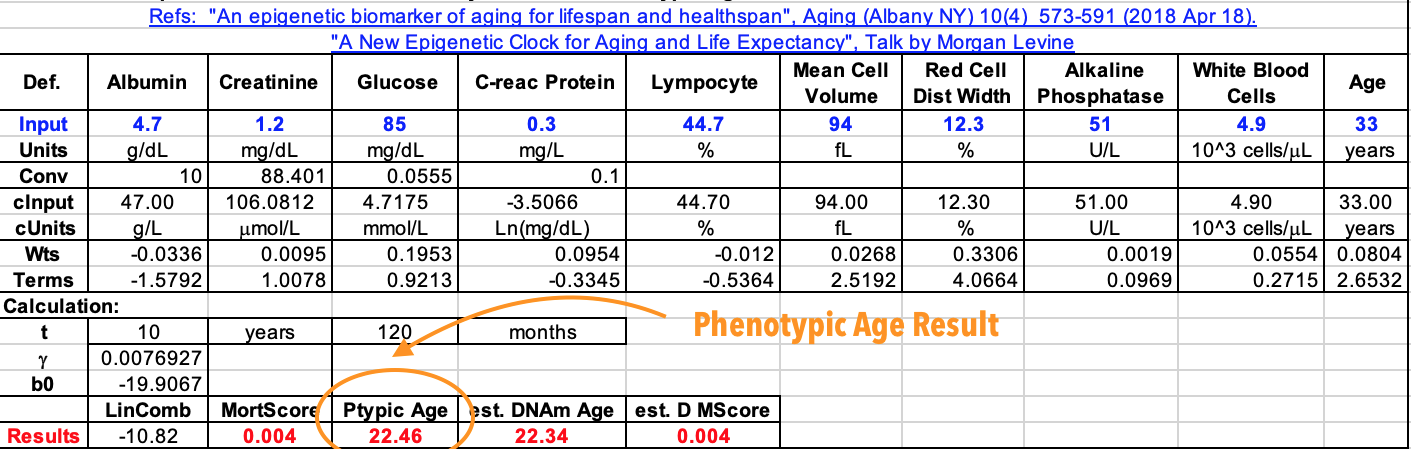
Biological Age Tool #2 - AgingAI
Another group of researchers who have pioneered biological age tools are the team at Insilico Medicine, developers of the ‘AgingAI’ tool. In fact, I considered Alex Zhavoronkov (CTO of Insilico) one of the world’s leaders in advocacy for longevity technology research, and if you are interested in this space, he is someone you should certainly follow.
AgingAI uses an artificial intelligence approach to biological age estimation, which is significantly more complex and technical than the linear model used in the phenotypic age tool. This approach employs deep neural networks and was trained on more than 60k data points (read more about the details here). In my view, this tool is inherently more subjective in that due to the machine learning approach employed, it will be biased toward chronological age more strongly than the phenotypic age model (simply put - the neural networks are trained against chronological age as ‘the answer’).
Using the results from my NextHealth Total Baseline I was able to complete both the AgingAI 2.0 and AgingAI 3.0 Tests. For those of you interested in replicating this with your own Total Baseline test, here are a few tips:
be sure to select “US” for the sample metric at the top
you won’t have a value for “Lactate dehydrogenase”, so I recommend using the median value of the reference range
“Basophils” is “Basos %”, “Eosinophils” is “Eos %”, and “Lymphocytes” is “Lymphs %”
in your Total Baseline report
And my results? AgingAI 2.0 guesses I am 30 years old. AgingAI 3.0 guesses 32 years old. Pretty close on both counts! And I suppose it is good news it knows I am a male (LOL).

Biological Age Tool #3 - RealAge by ShareCare
Not everyone will have the blood test results on hand to use both of the above tools (but you can likely get them if you find the right medical doctor! Also, read-on below, as it appears you can order these online via “Walk-in Labs”). So I wanted to make sure I included an age test that did not require a blood test. This one is arguably not truly a biological age tool, but I’ll place it in that category based on the amount of biological data it ingests through its questionnaire style approach (it does collect cholesterol numbers for example). Co-created by “Dr. Oz” and Mike Roizen, this tool boasts that is has been completed more than 43M times.

An example question from the RealAge survey tool
I appreciated this test for its accessibility and its candour. What I mean by the latter point is that it asks many questions that clearly gauge youthfulness through emotional and psychological data points (really digging into whether or not you still have that quintessential ‘zest’ for life or not!). It also provides a wide array of follow-up tools that directly target your RealAge score, and can help you improve it, including a ‘dashboard’ tool that will let you track your behaviours and give you tailored advice (and I am sure it will use your data to make money somehow!).
This test reported a ‘Real Age’ (biological age) of 28 years old.

Should you complete a Biological Age test?
If you’re interested in maximising your longevity, it’s important to establish a baseline. This means, to establish where your overall health and wellness are at NOW, so that you can make changes to your diet, lifestyle, supplements and other input variables, and then re-test to determine how you’re faring with your own longevity strategy.
In my view, biological age tests are an ideal choice of baseline testing, as they are designed to comprise the overall impact of many different factors and are specifically dedicated to measuring aging. However, there is a rapidly growing list of options for testing, including checking your telomere length (of white blood cells), DNA methylation clocks (e.g. DNAge), and more broad spectrum epigenetic tests (check out Chronomics for example). So selecting which test to use comes down to a few key parameters, in my view:
Representativeness of the test to your overall health & wellbeing (Does the age test capture the most representative biomarkers of aging?)
Affordability (Are you able to routinely repeat the measurement based upon its cost?)
Accessibility (Do you need a doctor to work with you to get the test? Is it available in your country/region? Can you order it online?)
As a part of my commitment to the purpose of this blog (supporting you in generating your own longevity strategy), I am preparing a review of several of the biological age tests available on the market, for publication on this blog later this year. By working with the providers of these tests, I’ll share my results with you, and compare and contrast the (1) representativeness, (2) affordability and (3) accessibility of each approach. In this post, we got off to a solid start, so let’s close today by summarising these three factors for the above biological age tests in a succinct tabulated format. I will be sure to update this table as I evaluate additional options in the future!
![Costing estimates produced with “Walk-in Labs” [1], [2], [3]. My total baseline test cost $999USD.](https://images.squarespace-cdn.com/content/v1/534cff75e4b0ce1c16de5321/1578708035056-NQBT0PVSD7FSR14BJDYH/Aging+Tests+Matrix+v1+January+2020)
If you enjoyed this post, be sure to read my coverage on epigenetic age testing company Chronomics

Want to test & improve you biological age? Longevity Blog recommends GlycanAge
Our Founder Nick used these kits to improve his biological age by 6 years, just by changing his diet. Read more about that here.
If you’d like a more robust and accurate biological age test than the free options above, GlycanAge is a great place to start!
-
RT @rebeccavziegler: The cryonics payoff matrix. Choose wisely my friends. https://t.co/l1rzsmOC2w
-
My rate of aging: 0.79 It’s the new street cred What you got? https://t.co/aHzWHAfCnD https://t.co/L3rZC4QFN2
-
It’s official - I’m co-producing and hosting a new #longevity docuseries, and will begin shooting in a few months… https://t.co/wLGqRrBfbp
-
“The #longevity segment opened my eyes to the groundbreaking advances in biotechnology, health, and wellness. The i… https://t.co/F8YB7PAeMW
-
I’m completely mindblown by what AI has done over the past 3-6 months, and it continues to accelerate… https://t.co/hh0JslucRg
-
Longevity legends take on many shapes and sizes https://t.co/X9vGa7gvOe
-
RT @BradStanfieldMD: Avoid These Popular Supplements (shout out to Professor Matt Kaeberlein @mkaeberlein & Professor Brian Kennedy… https://t.co/cy9CXldgUS
-
Who are influential persons in #longevity who are of Asian, African American or other “minority” group in the US?
-
The AI powered future is here 🦾 Contrary to the narrative, you’re not going to be replaced in the workplace by AI… https://t.co/BojTzyfDzA
-
I built and exited my first company today A big moment in my entrepreneur journey What’s next? All in on… https://t.co/5oTo3IjSyN

Immediately actionable insights via micronutrient testing
Considering a micronutrient test? Do these two things first!
Want to take a micronutrient test? Order your own without a doctor!
Micronutrient test results are in!
Imagine my excitement as the moment finally arrived - the comprehensive results from my 15 vials of blood and four detailed blood tests arrived in my inbox. After 4 weeks of waiting, the mountain of data arrived and the real fun of digging through it for actionable insights began. To get started, I’d like to share with you three immediately actionable insights I gained from my micronutrient blood test.
Micronutrient test for Glutamine (actionable insight #1)
Huffing and puffing my way towards my cardio goals (I plan to run my first 10km race this year) sure leads to a lot of SWEAT. Much more than I’ve personally been used to. I’ve established a solid routine where 6 days/week, I am up early in the morning getting in a vigorous walk of 5k+ steps or run workout (trail runs, endurance training - follow me on Strava). However, unbeknownst to me, that SWEAT was taking with it a critical micronutrient needed for the success of many different bodily systems - Glutamine.
Glutamine is an amino acid that plays a critical role in the synthesis of proteins, which has impacts for many bodily systems. In fact, it is the most abundant amino acid in the human body. This being the case, it is also abundant in a wide variety of our food choices - including meats like beef, chicken and fish, dairy products, eggs, and many vegetables (leafy greens, carrots, cabbage, beets).

After a deep dive on all the best options, I opted for this L-Glutamine powder from California Gold. They also offer a capsule form. Save 10% and support the Longevity Blog with code EYU021
But my levels were low, as in rock-bottom low, and that had many knock-on effects to my neurological function, gastrointestinal barrier, my liver performance, my joint health, my skin vitality and my mitochondrial function. Just check out the useful summary graphic provided in my report (the one with the multiple indicator “gauges”, note that you can click on the image to see the full size)
Low glutamine is simply put - bad news. For a young and healthy person looking to optimise his wellbeing and longevity, this was certainly limiting my performance. For some perspective on just how low my levels were, check out the reference ranges in the next image. The ‘Serum’ levels (what was detectable in my blood liquid - not the actual cells) was only 23.6 nmol/mL! Thankfully, the amount in my white blood cells (WBC), which is an indicator of long-term micronutrient availability was in the normal range, but the serum level was nonetheless quite problematic.
Needless to say, I jumped on a high quality glutamine supplement from my brand of choice (California Gold - save 10% and support Longevity Blog with code EYU021 ) within a few days. I immediately enjoyed a noticeable improvement in my gastrointestinal health, with knock on effects to the health of my skin (less acne breakouts) within just a few days. The bottom line here - this was incredibly valuable and highly actionable information that was available to me through this micronutrient test.

Micronutrient test for Chromium (actionable insight #2)
My glutamine levels weren’t the only important micronutrient that was critically low, as my intense levels of exercise and SWEAT were also depleting an important mineral - Chromium. Further research revealed that Chromium is commonly deficient in athletes for this reason.
Chromium plays a very important role in metabolism, and is directly involved in the breakdown of fats and carbohydrates. With respect to fats, it stimulates the synthesis of cholesterol and fatty acids. For carbohydrates, it is involved in the regulation of insulin. It also is involved in the metabolism of some amino acids. Once again - very important!

I took a pretty picture for you! Chromium Piccolinate to the rescue!
Dietary sources of chromium include broccoli and green beans (which I eat daily!), meats like beef and poultry, and fruits like apples and bananas (which I regularly also enjoy). However these dietary sources are still relatively low.
This makes chromium supplementation a well-informed choice for me and for anyone else who is moderately active (or wants to better manage their insulin levels, e.g diabetics), which is the second immediately actionable insight I garnered from my NextHealth micronutrient test. I turned to my vitamin supplier of choice - Thorne for a Chromium Piccolinate supplement, but later pivoted to the cheaper version from Now and take it twice a week with my Vitamin C and B-vitamin complex to improve absorption. Just like with the Glutamine options on iherb - use the discount code EYU021 to save 5% and support the Longevity Blog!
Micronutrient test for Vitamin K1 (actionable insight #3)
There are two forms of the fat-soluble vitamin K needed by the body - K1 and K2. These are important for blood clotting, regulation of calcium (particularly bone metabolism) and cardiovascular health. Vitamin K also plays a role in mitochondria producing energy for your cells.
It also turns out, that despite plenty of dietary intake of Vitamins K1 and K2 in my vegetable rich diet, my micronutrient testing revealed critically low amounts of Vitamin K1 in my blood serum. Additionally, despite my 100mcg/day supplementation of K2, it was also fairly low. This clearly made supplementation of Vitamin K1 (and continued supplementation of K2) the third immediately actionable insight gained from my micronutrient testing at NextHealth.

Conclusion - Micronutrient testing is a valuable, actionable tool
There is so much more that I gained from my micronutrient testing that I hope to share with you in upcoming posts (be sure to subscribe to the Longevity Blog!), including my Omega 3/6 balance, copper-zinc ratio and antioxidant levels. However, even without these added benefits, I believe the outcome of my first micronutrient test is clear - regular assessment (I’m guessing every 6-months) of one’s micronutrients provides actionable insights that can be used to improve your health and optimise longevity.
I’d like to close with my sincere thanks to NextHealth for living up to their mission as a Health Optimisation and Longevity Center, and making is simple, straightforward and affordable to access this resource. I’ll certainly be back for my next micronutrient test in 2020!
Follow-up Post: Considering a micronutrient test? Do these two things first!
Ready to test your micronutrient status?
We’ve found three valuable DIY options for you! No doctor required!
HealthLabs USA)
UltaWellness (USA)
I-Screen (Australia)
-
RT @rebeccavziegler: The cryonics payoff matrix. Choose wisely my friends. https://t.co/l1rzsmOC2w
-
My rate of aging: 0.79 It’s the new street cred What you got? https://t.co/aHzWHAfCnD https://t.co/L3rZC4QFN2
-
It’s official - I’m co-producing and hosting a new #longevity docuseries, and will begin shooting in a few months… https://t.co/wLGqRrBfbp
-
“The #longevity segment opened my eyes to the groundbreaking advances in biotechnology, health, and wellness. The i… https://t.co/F8YB7PAeMW
-
I’m completely mindblown by what AI has done over the past 3-6 months, and it continues to accelerate… https://t.co/hh0JslucRg
-
Longevity legends take on many shapes and sizes https://t.co/X9vGa7gvOe
-
RT @BradStanfieldMD: Avoid These Popular Supplements (shout out to Professor Matt Kaeberlein @mkaeberlein & Professor Brian Kennedy… https://t.co/cy9CXldgUS
-
Who are influential persons in #longevity who are of Asian, African American or other “minority” group in the US?
-
The AI powered future is here 🦾 Contrary to the narrative, you’re not going to be replaced in the workplace by AI… https://t.co/BojTzyfDzA
-
I built and exited my first company today A big moment in my entrepreneur journey What’s next? All in on… https://t.co/5oTo3IjSyN
FDA & TGA DISCLAIMER
This information is intended for educational purposes only and is not meant to substitute for medical care or to prescribe treatment for any specific health condition. These blog posts are not intended to diagnose, treat, cure or prevent any disease, and only may become actionable through consultation with a medical professional.

Time travelling with the health nucleus: Ancestry in your DNA
Time travelling with the health nucleus!
This post is a personal entry from our Founder Nick
I have always found it fascinating to ask the question - ‘where have I come from?’. Not in terms of where I have lived or the birds and the bees - no I refer to the much grander scheme of things.
Each of us is the product of a man and woman who have combined their DNA to create offspring, and on a broadly twice decadal time scale, a new generation in our lineage appears. A multitude of factors have come together to make this so, right down the particular genetic information carried by the sperm and egg cell that made the action happen!
Exploring ancestry with my 84 year old grandfather
I recently visited with my 84 year old paternal grandfather, who has created meticulous records of the family genealogy, reaching back into the late 1800s. It was just after the US civil war when my great, great, great grandfather John immigrated from Bavaria, Germany to Bay County, Michigan.
It’s just one more story in the treasured history of European immigrants arriving on the shores of the United States to form new communities and create new opportunities in America.
Stories like this one, fill my heart with awe and wonder in their romanticism. But that’s not exactly what this blog is about now, is it?
While I might find this story elegant and inspiring, what I find much more interesting and actionable is what it tells me about my genetic heritage, and how I might further optimise my own life based on my own genome.
And until recently, anecdotes like the ones my grandpa compiled were the only good information we could access on this topic.
Whole genome sequencing at the health nucleus fills in the blanks
In May 2018, as I previously blogged, I had my first (and certainly not my last!) visit to the Human Longevity Inc. “Health Nucleus” in San Diego. One part of this amazing experience, was the drawing of blood to sequence my whole genome.
To be clear, this is not the same sort of tests you can get from “DNAfit” or “23andMe”, which look at only certain parts of the genome. While such tests can provide valuable and actionable data, what I had completed for myself is something only a few thousands of people around the world have done to date! But given the recent falls in cost for having this done, that’s sure to be quickly changing….
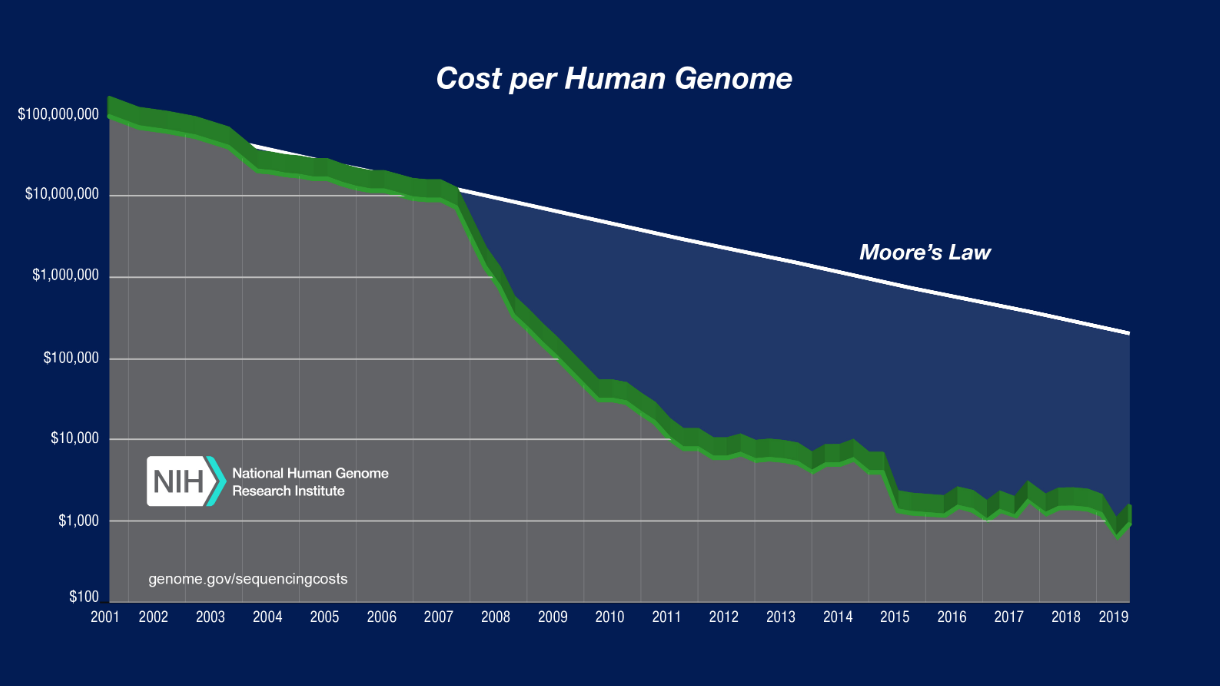
Whole genome sequencing refers to the process of analysing the full sequence of human DNA, which is more than 3 billion base pairs in total! Specifically, ‘Whole’ genome sequencing includes both chromosomal DNA and mitochondrial DNA.
What did I learn sequencing my whole genome?
Did you know? While whole genome sequencing is still pretty expensive, you can still analyse over 700k locations of your DNA with Self-Decode for less than $100!
I am still sifting through the 400+ page report that reviews all of the results and insights that I gained from sequencing my whole genome.
With 3B base pairs of information, we are still learning what each of the many variations in each of our DNA actually mean.
Many of the results I received were actionable (e.g. my cardiovascular and alzheimers disease risk - more on that in future posts!), some were less valuable (e.g. my genetic disease risk - I would have already known by now if I had one of these conditions), and others were just downright fascinating.
And that’s what loops us back around to the stories and history that my grandfather had worked so very hard to compile.
He had spent countless hours researching, documenting and sharing these precious pieces of information, and still had only managed to reach back about 150 years in time.
But just imagine you could look even further. What could a thousand years of genetic history reveal? How about 10,000 years? 65,000 years or more? Is such an analysis possible? If so, what could it teach one about themself? And moreover, could it help them biohack their way to a long and healthy life?
Autosomal ancestry
First, let’s look at my autosomal ancestry determination. Autosomal DNA in genetic genealogy is used to describe the 22 pairs within the chromosome that are independent from the X and Y sex chromosomes. I won’t delve into it further here, as that is not my role.
I suggest you use the most excellent ISOGG Wiki if you want to go deeper!. Autosomal ancestry compares your genome to other genomes from different populations of known origins, and is most relevant for your genetic ancestry on the order of 100s of years in the past.
The Health Nucleus report provided me with two related images to this analysis, both of which have largely confirmed that hard work my grandfather completed!
But of course, it also collated the results from my maternal grandparents and paternal grandmother as well (which were not included in his hard work!).

Autosomal DNA analysis confirms - yep, German! And maybe a spot of English in me too ;)
Haplogroup exploration via my paternal chromosome
Hey, that was neat, but we kinda knew that information already. After all, I am white guy who likes beer.
Can we go back further? Yes we certainly can! The next tool for diving into ancestry are “Haplogroups”. ISOGG defines a Haplogroup as follows:
“A haplogroup is a genetic population group of people who share a common ancestor on the patriline or the matriline. Haplogroups are assigned letters of the alphabet, and refinements consist of additional number and letter combinations.”
Haplogroups can help identify the origins of your ancestors dating back on the order of thousands to tens of thousands of years! Common ancestors can be explored through both on the patrilineal (father) or the matrilineal (mother) histories.
Here we are looking into the sex chromosomes (as opposed to the autosomal regions above). Looking at my Y chromosome follows my father’s history, and this information will be shared by both my brother and my son (how cool is that?).

From my report:
“Your Haplogroup is: G2a1c2b1a. Haplogroup G is from approximately 48,000 years ago and is found in low frequencies in north Africa, north and west Asia, Europe, India, Malaysia, the Middle East, and Sri Lanka. It possibly had a period of isolation for over 10,000 years in southwest Asia.”

This beer drinking guy from Germany just had his mind blown! 10-50kya my ancestors were likely from modern day Turkey or Georgia! And since this is a Y-chromosome based analysis, that information is relevant to my son, my father, and even my 84 year old grandfather. I can’t wait to send him this blog!
Mitochondrial DNA haplogroup analysis
Mitochondria have been on my mind a lot lately. They are quite fascinating and turn out to be very important in the ageing process itself (for example, did you know - damage to mitochondrial DNA is one of the key reasons we age?). mDNA is inherited only from the mother, and therefore gives us the opportunity to look down my maternal genealogy. All of my biological siblings (we share the same mother) will have the same mDNA haplogroup, however my son will not, as he will have the mDNA of my wife.
From my report:

“YOUR HAPLOGROUP is: U5b2b3 Mitochondrial haplogroup U is estimated to have originated approximately 55,000 years ago. It has been identified at high frequencies in North Africa, Central and South Asia, the Middle East and Europe, where it is the oldest and predominant haplogroup.”
This analysis seemed to have much less confidence, as it spans from northern India, across parts of the Middle East and into eastern Europe, so I don’t quite know what to make of it at this stage! I’ll have to do some more digging around to see if I can narrow this down any further to make it more targeted.
Lastly, I am part neanderthal (and my wife is not surprised)
Hey guys, fun fact. I am 1.72% Neanderthal and only 98.28% Homo Sapien… 😮

OK, so this is not unusual as the typical range is 1.4% to 2.1% for Europeans. But I left you hanging for a minute and that was fun 🤗.
So - is this data actionable?
A key question I like to ask on this blog is - is the data action actionable? With respect to the ancestry analysis, I conditionally believe that it is.
This ancestry analysis tells me information about the environment that my body has evolved in response to, and offers hints to the diet that my ancestors likely consumed. Both of these are very influential aspects in the longevity journey.
For example, it may reinforce my routine use of cold exposure (cold showers, ice baths, cryotherapy), as it is clear from my autosomal analysis and haplogroup G categorisation that many of my ancestors were not the types to lounge in tropical climates, but instead would have seen hard winters.
They would have marginally evolved on the order of tens of thousands of years in response to those conditions.
Speaking of cold winters, I add an additional presumption that my body would likely favour some level of fasting and primarily carnivore/ketogenic diet for a certain portion of the year, based on what we’ve found here.
Additional insights could be gained by researching what these haplogroups have been discovered to eat in the past. But that is all research for another blog post and another day :). Trust me, I’ll get there. I’m too damn curious not to!
In closing, I would like to suggest that any of the above assumptions about environment and diet should be paired with further analysis of my genome sequencing results (e.g. like the Genomic Fit test I just completed at NextHealth!).
I should also note that given our increasing understanding of the role of the epigenome in expressing our genomic information, that the impacts of my current environment, diet and lifestyle also have a role to play in making conclusions about further biohacking and ’optimisation’ of myself.
This stuff is complicated and highly non-linear, but hey, bringing you guys along on this journey so we can sort it out together, is what this blog is all about.
-
RT @nickengerer: Join a team, do a sport. Staying fit is easier with a clear purpose Bonus: you just might live longer Pic: Byro… https://t.co/L5yHxHJXas
-
Calcium AKG Alpha Keto Glutarate Supplement Review https://t.co/K7keDM3Lyn
-
Mitopure Review - Does this Urolithin A supplement actually work? https://t.co/0Y6Bx4yA7h
-
How Fast are You Aging? A Biological Age Test for Rate of Ageing with Ryan Smith of Trudiagnostic (Part 2) https://t.co/5SZW3Or6JJ
-
What is the Most Accurate Biological Age Test? An Interview with Ryan Smith of Trudiagnostic (Part 1) https://t.co/wdIxtTVeq0
-
One Skin Review - Self-Experiment Before and After Results with OS-01 https://t.co/3hqzLtfVa3
-
Regrowing Knee Cartilage and Restoring Joint Health Naturally. An Interview with Reviiv Light CEO Forrest Smith - P… https://t.co/O671LROvzw
-
RT @nickengerer: 90 years old, what to do? A half Ironman, why not? Hiromu Inada now holds the record for the oldest ever competi… https://t.co/wv7NPhslUM
-
One Skin Before and After - Skin Aging in the Future: An interview with OneSkin CEO Dr Carolina Reis - Part 2 https://t.co/RlLlqRurT6
-
RT @Do_Not_Age: Our new ingredient, Spermidine, reduces amyloid plaques and inflammation of the brain in rodents Check our Science… https://t.co/RgehOqmVtf
Body composition data - Tracking lean muscle mass and fat over time
InBody and Styku body scan technology - Is it actionable?
While we are (im)patiently waiting on the results from my blood tests at NextHealth, let’s take a look at another longevity and wellness datapoint that I was able to collect during my recent visit. In my meeting with my “Health Coach” at NextHealth, we completed two types of body composition scans. The first was an ‘InBody’ scan which uses bioelectrical impedance to estimate:
Total skeletal muscle mass
Total body fat in kilograms
Total body fat percentage
Visceral fat
As well as make estimates of your basal metabolic rate and a few other body composition items.
The second was a a Styku which actually uses an Xbox Kinect and a rotating platform to create a full 3D scan of your body.
A key question that I have for these types of body scans and body composition data overall is - “Is this information actionable/valuable?”. In this post, I’ll aim to answer that question from my perspective.
Let’s dive in and take a look at some results!
Comparing my InBody scan across 18 months
The biggest value in body composition data lies in tracking how it changes over time. On shorter timescales of months to a year, you are able to track how your diet and/or exercise routines are affecting your lean mass, fat mass and/or visceral fat values. Over longer timescales, on the order of several years, you may even be able to track the impacts of aging on your body composition (e.g. the loss of lean muscle mass as the years stack up - yikes!).
I did my first InBody composition scan at the Health Nucleus in May of 2018. At the time, I was about 11 months into a year-long experiment eating a (very clean, whole foods based) ketogenic diet. I was doing an above average amount of physical activity (12k steps/day), but was not ‘working out’ or completing any cardio exercise.
However, that has all changed significantly. As I recently wrote, one of the key outcomes from my visit to the Health Nucleus was a life-long dedication to cardio fitness! So in the 18 months since my first InBody scan, I had added several days/week of cardio training (mostly running), and some strength training (still working on adding more of this), and I had returned to a whole-foods, carb-based diet (retaining plenty of healthy fats). One additional factor on the diet front has been my experiment over 2019 of water-only fasting for 2-4 days per month.
What did my two InBody scans show (before & after)?
“As you can see here”, Sirish the health coach pointed out with his pen, helpfully marking up my scan results, “Your body is actually pretty symmetrical from left to right. That’s not actually very common”.
I was immediately pleased. Symmetry was something I had been working on religiously, aiming to correct the imbalances I had in my body from left (weak) to right (strong), particularly in my running stride and strength workouts like push-ups.
“Your lean body mass is 157lbs (71kg), and with a total body weight of 177lbs (80kg), that places you at 10.7% body fat, which is at the low end of the normal range”, he commented. “We will get some further detail on this with the Styku body imaging data next”.
“That’s great mate!”, I responded. “That’s actually about the same number I get on my FitBit scale at home”. It was a solid ‘calibration’ of my in-house data, which is very useful.
In the following images (you can click through using the embedded controls), I have add some call-out annotations to draw attention to some actionable insights from my reports.
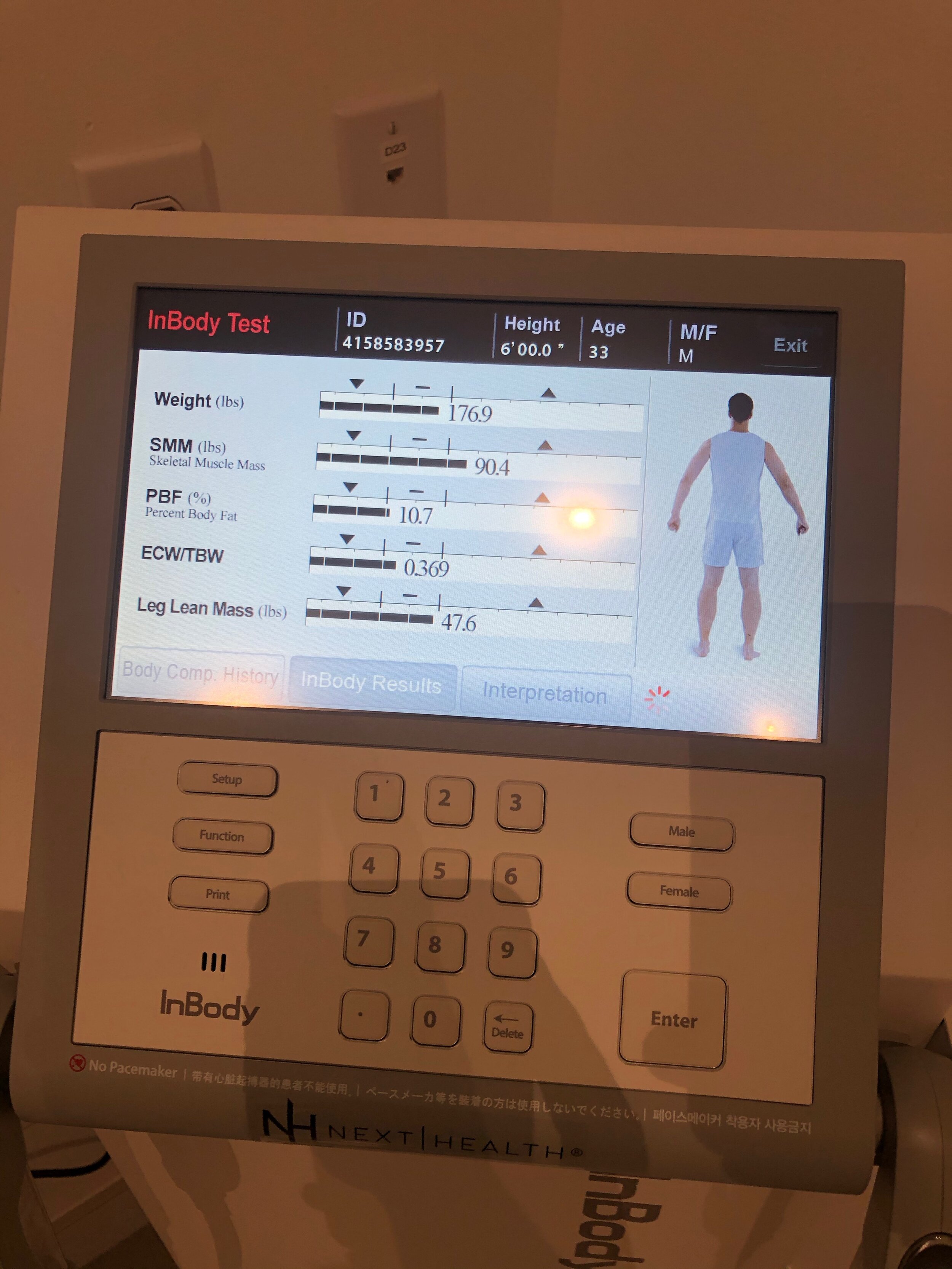
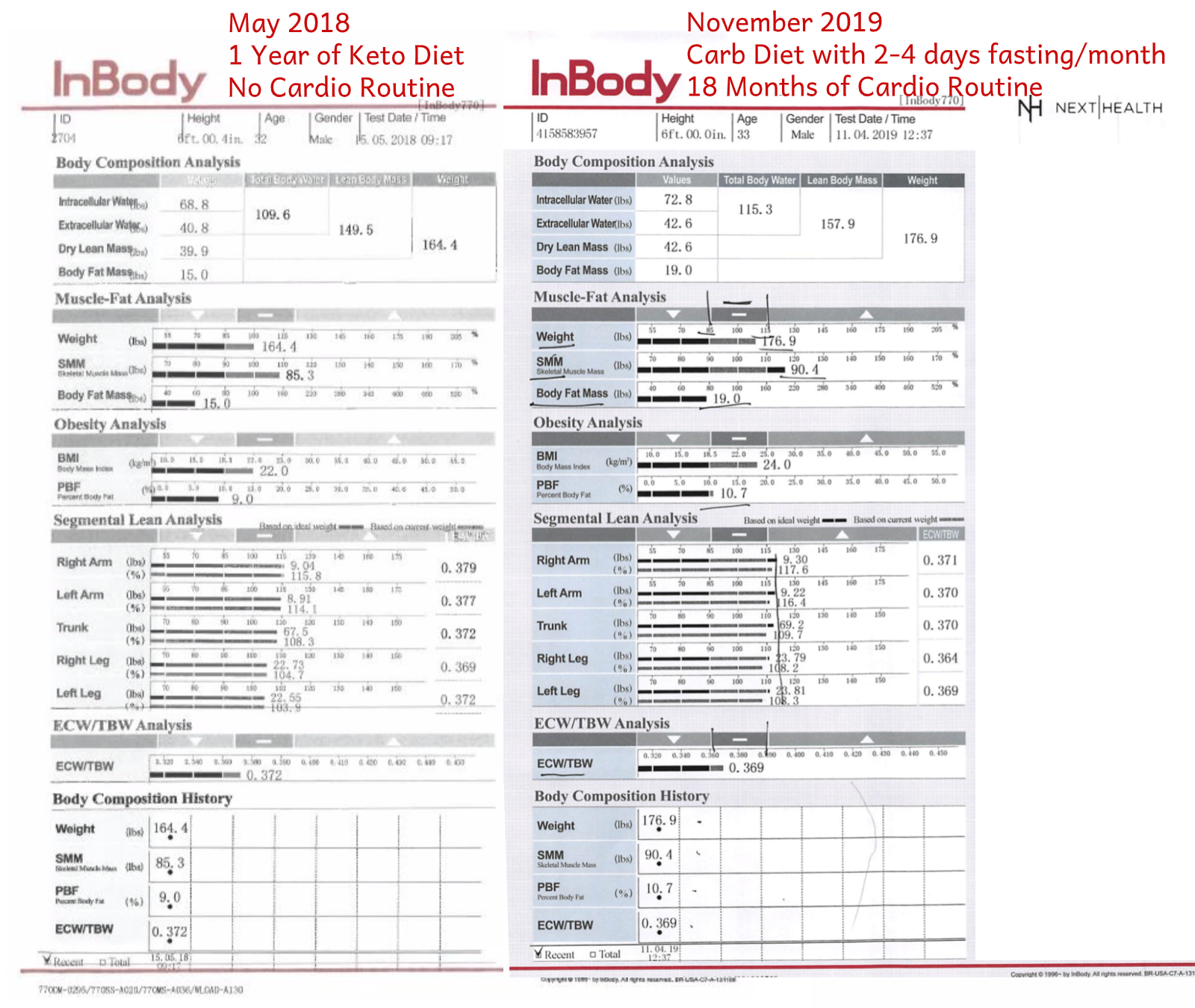
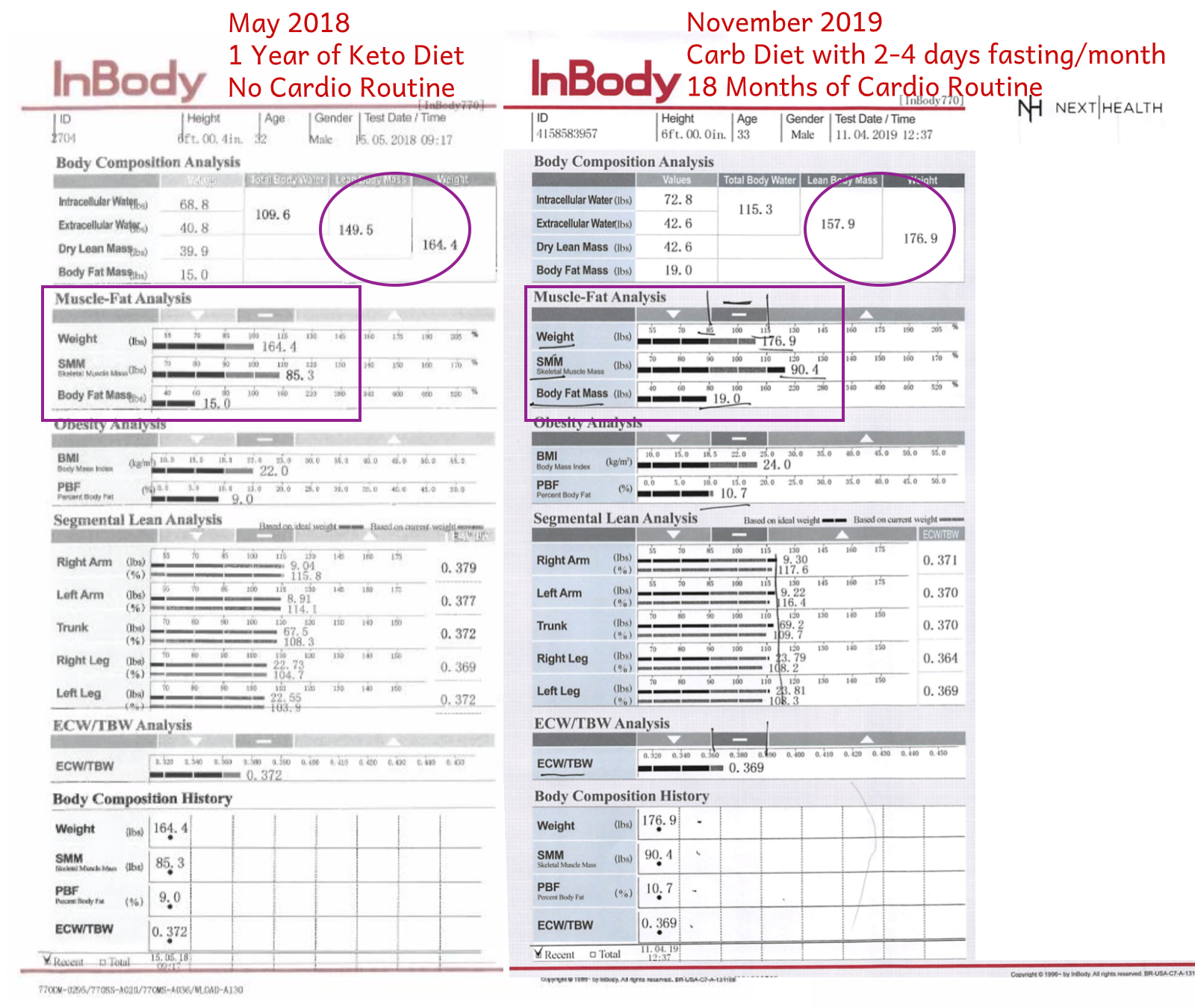
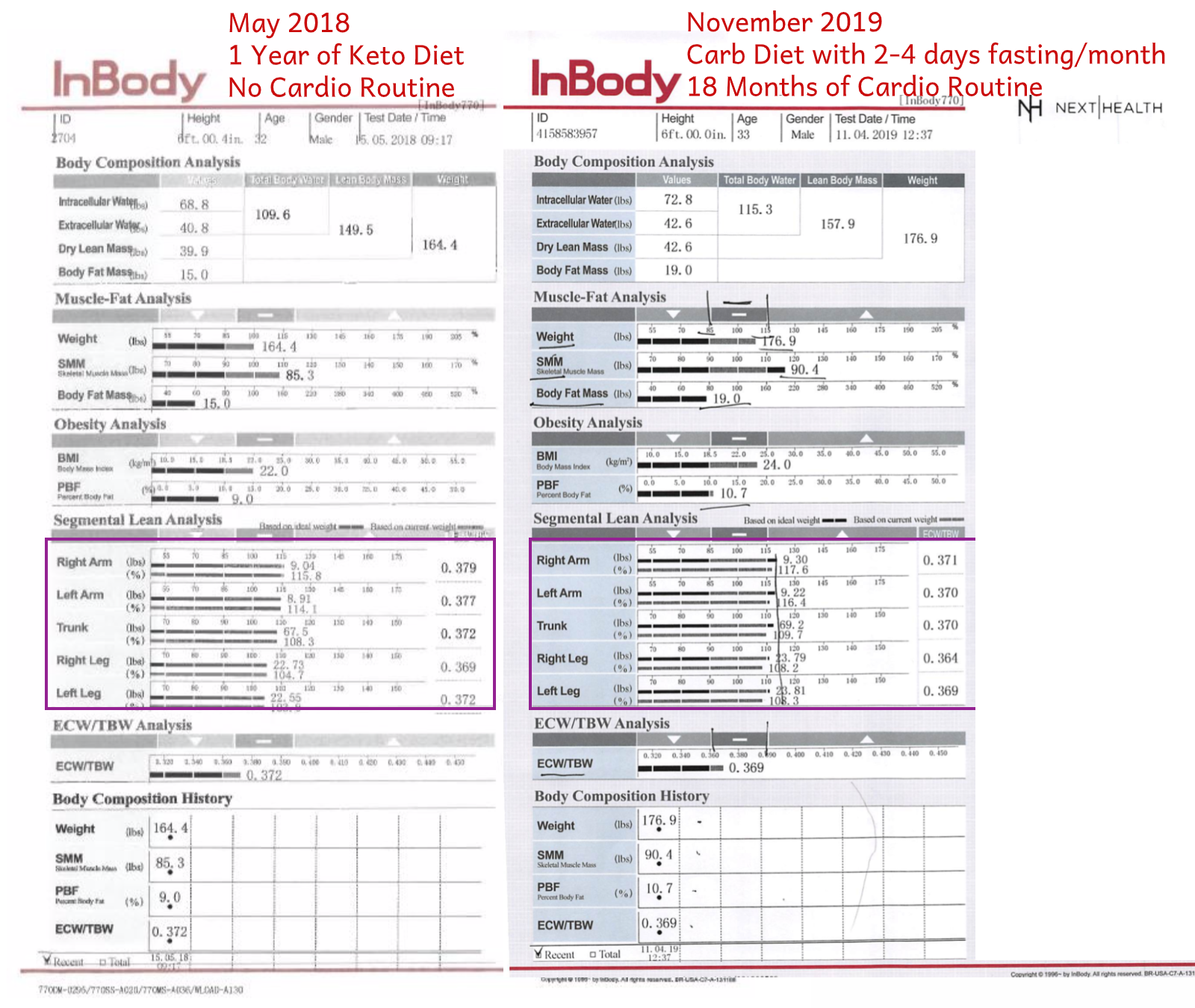
Conclusion: The InBody scan can definitely provide you with actionable data. Knowing where you stand with respect to your visceral fat mass alone is hugely valuable for assessing your disease risk For me, it was able to provide evidence that changes in my diet and exercise routine had contributed positively to my lean body mass. It also provided me with evidence that my efforts to increase symmetry in my body were fruitful and worth maintaining.

A Styku Haiku
One spinning platform
I stand upon with arms spread
Where did my hand go?
Styku body imaging
“Go ahead and strip down to your underwear and jump on this platform.”, Sirish beckoned, “I will step outside until the scan is completed”.
“Naw, mate. I couldn’t care less if you stick around!”, I explained, as I jumped upon the pedestal and started a slow rotation with my arms spread wide. Hey, it was just another day at NextHealth, where between the Cryo, the Infrared Sauna and Instagram, everyone’s half-naked most of the time anyway 😉!
Nudity jokes aside, the Styku scan provided some damn good data! Superceding the InBody scan with its detail, the Styku scan reported on the individual components of the legs, arms and trunk. Despite the accidental truncation of my left forearm (oops!), I was able to get a fairly comprehensive set of data points regarding my lean muscle mass distribution across the body.
Conclusion: The Styku data was certainly actionable. For example, while I had great symmetry in my thighs from left to right, the Styku was able to detect and measure asymmetry in my left and right calf muscles. I now will be adding some additional hypertrophy exercises to that lagging left calf muscle, and hopefully this will lead to performance gains in my race times!
Detailed Styku esults:
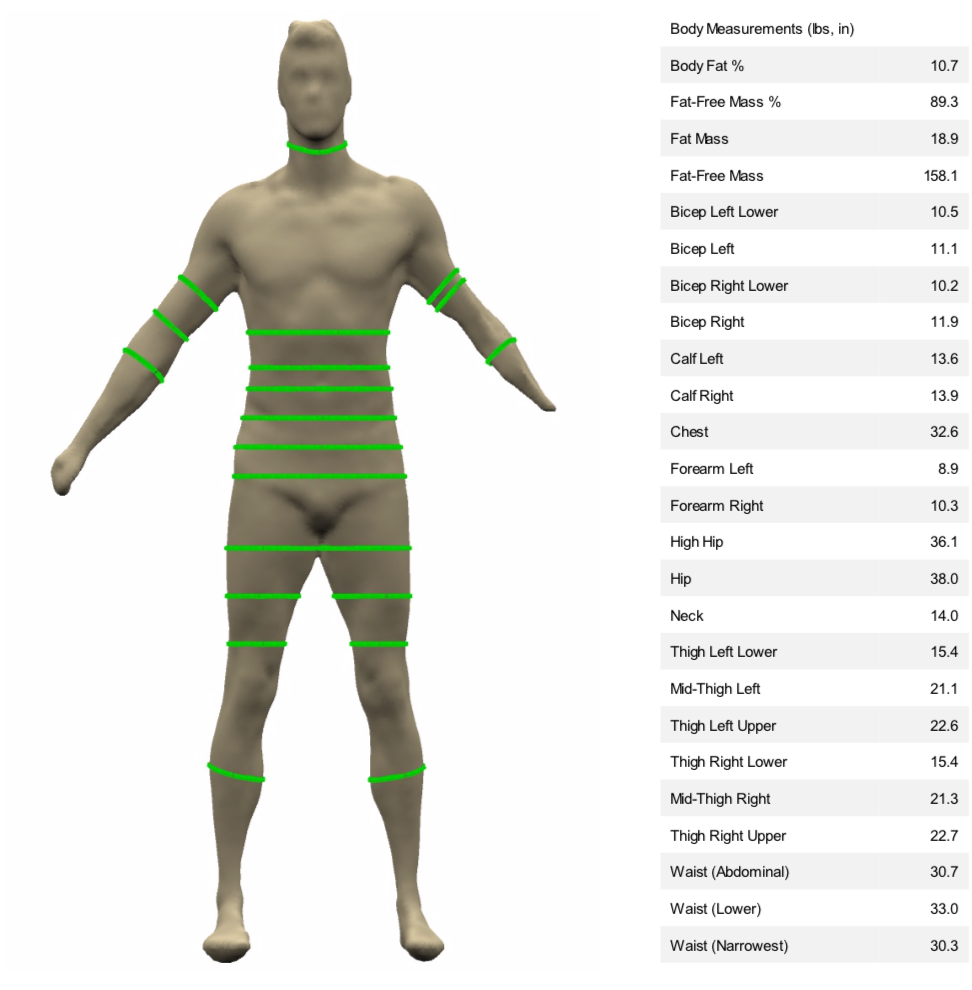



Body scan data is actionable - But blood markers will be even more exciting
Overall, I believe that this type of body scanning data is valuable for folks like me, who are trying to optimise their body and mind, relentlessly (hey that’s what being a biohacker is all about!). It may have additional benefits for folks who are overweight/obese, as it can highlight their elevated risks from carrying high amounts of visceral fat. I plan to continue tracking my results with both the Styku and the InBody tools on a yearly basis (and of course I will share what I learn on this blog!).
Body composition discussions aside, I only have to wait a few more weeks until I get the results from the 15 vials of blood I gave to NextHealth. I’m totally jazzed about this, and can’t wait to share what I learn from detailed analysis of my blood. Be sure to subscribe to the blog below to get notified whenever I add new longevity, healthspan and biohacking focused content!


-
RT @rebeccavziegler: The cryonics payoff matrix. Choose wisely my friends. https://t.co/l1rzsmOC2w
-
My rate of aging: 0.79 It’s the new street cred What you got? https://t.co/aHzWHAfCnD https://t.co/L3rZC4QFN2
-
It’s official - I’m co-producing and hosting a new #longevity docuseries, and will begin shooting in a few months… https://t.co/wLGqRrBfbp
-
“The #longevity segment opened my eyes to the groundbreaking advances in biotechnology, health, and wellness. The i… https://t.co/F8YB7PAeMW
-
I’m completely mindblown by what AI has done over the past 3-6 months, and it continues to accelerate… https://t.co/hh0JslucRg
-
Longevity legends take on many shapes and sizes https://t.co/X9vGa7gvOe
-
RT @BradStanfieldMD: Avoid These Popular Supplements (shout out to Professor Matt Kaeberlein @mkaeberlein & Professor Brian Kennedy… https://t.co/cy9CXldgUS
-
Who are influential persons in #longevity who are of Asian, African American or other “minority” group in the US?
-
The AI powered future is here 🦾 Contrary to the narrative, you’re not going to be replaced in the workplace by AI… https://t.co/BojTzyfDzA
-
I built and exited my first company today A big moment in my entrepreneur journey What’s next? All in on… https://t.co/5oTo3IjSyN

Why I Just Gave 15 Vials of Blood at NextHealth
Visiting NextHealth in Los Angeles to See and Experience Proactive Healthcare in Action
I’m coming off a real high having just been to LA and San Diego over this past week and not just because I had my face bathed in some awesome infrared radiation with a “Light Stim” (see this IG post and be sure to give me follow 😉). No, I’m jazzed because I FINALLY visited NextHealth in Century City, LA - and let me tell you, it was a life changing experience!
What is NextHealth?
NextHealth refer to themselves as a “Health Optimisation and Longevity Center” - as you can imagine, I fit quite squarely into their market segment (I am trying to Biohack my way to a vibrant, healthy, long life after all). They do everything from cryotherapy to dermatology and IV vitamin infusions to blood testing.
Why Did I Visit NextHealth?
This time I was out for blood 💉!!
NextHealth offers a few blood test products that I was very interested in for supporting my longevity journey. These are:
And then, upon further digging into some other options during my visit to the site, I decided to also add on:
My Motivation: Get Feedback and Optimise
There is simply no way to start to introduce all of the different things that will be covered by the above blood tests, those are quite extensive! But I do have a select number of things that drew me to these blood test options, by blood test product they are:
Total Baseline:
I was very interested in my NMR spectroscopy results so I can better understand what the particles sizes make up my LDL cholesterol
I am in my early 30s and undertaking many ‘hacks’ to keep my testosterone high - are they working? (dutch test hormone data!)
Micronutrient Testing
I have an aggressive supplement regimen (30+ supplements a day and climbing), and micronutrient testing will help me adjust the levels of supplementation very accurately
Genomic Fit
I am interested in optimising my diet and athletic performance (going for a sub-20 minute 5K at the moment) and ‘Genomic Fit’ will give me some actionable info on this
Food Sensitivity Testing
Figuring what foods you are sensitive to (different from being allergic) is very difficult to do with dietary testing alone, and I can tell I still have some foods in my diet that give me inflammation - what are they? I must know so I can ban them and protect my gut lining!
All Up I Gave 15 Vials of Blood in the Name of Science




“It’s less blood than it looks like”, Ashley, the gorgeous phlebotomist let me know. “We’re almost done”
Good, cause I was totally light-headed already.
“Yeah, I passed out once when I gave about 30x vials for a scientific research study”, I let her know. “But don’t worry, I totally gave that nurse a heads up that I was on my way out”, I joked.
She just laughed and smiled re-assuringly (and probably thinking “God, don’t let this guy fall over on me…”). Thankfully Nick stayed conscious this time, and just like she promised - the blood draw was over quite quickly.
And might I say - it was an exceptionally professional job done on the blood draw, complete with a comfortable chair and warm-up blanket over the arm to kick it off. A smoother experience than I have had in many hospitals!
While I’m Waiting for the Blood Test Results…
I am not going to get my blood results back until early December, so this story is far from reaching its conclusion. In fact that visit to NextHealth was so life-changing, I easily have 10-15 more blog posts I’d like to write about it.
One thing is for sure, I will have plenty of material to work with. I once again am going to find myself with a stack of amazing health data to dig through! It is my plan to walk through some key lessons I learn from those blood results in upcoming blog posts, so be sure to subscribe to the blog if you’d like to see what happens!

Exercise and longevity are inseparable
Aerobic exercise is must have for longevity
Nick shares a personal story from his Health Nucleus journey in 2018
“Before I came into work to meet you here today, I got in a 40 minute run along the oceanfront”, Dr. Sanders said “I have made it a priority to get in at least four workouts per week, aiming for five or more.”
I sat and listened attentively, as she reviewed my intake questionnaire - noticing my history of high-ish blood pressures and LDL cholesterol values. Dr. Sanders was in her 40s, blonde and super fit - totally unlike any other doctor I’d met along my health journey. Simply put - she clearly walked the talk.
“I recommend you aim for 30 minutes of vigorous physical activity a few times a week. There is hardly a better preventative medicine in our toolbox than that.” she explained. “It can be hard to make a change, but trust me, it will help you with your blood pressure, blood lipids and insulin sensitivity.”
As I took this instruction in, sitting the Health Nucleus guest room (in my awesome socks), I realized I had a bit of reckoning coming my way - I’d come all this way for the latest in all things ‘proactive healthcare’ (full body MRI, genomic sequencing, full blood tests) only to be told, once again, I needed to get more ‘cardio’ exercise. Ugh.
Gasping, sweating, tiring - I’d never really ‘connected’ with the practice of this genre of fitness. I’d had a long-time love for weightlifting, and had dabbled in amateur sports such as flag football and softball.
I’d even enjoyed the occasional cardio-class after an arm-twist from a friend. But that’s not what she was suggesting - this was an overhaul of my life.
To be honest - it didn’t feel immediately doable.
Want longevity? Exercise delivers
As I hopped on my plane flight back to Australia from that amazing visit to San Diego, Dr. Sanders’ instruction really stuck with me.
I’d travelled half-way across the world, driven by my ever-growing interest in the fast moving world of longevity and healthspan, enthusiastic about gathering data and personalised guidance for living my best life.
And while many exciting longevity boosting technologies are indeed on their way quite soon (senolytics, gene therapy, stem cell treatments and more!), Dr. Sanders has made it very clear - you can’t avoid nailing the BASICS, which are tried and true, available here and now.
Exercise and a healthy diet form the foundation of wellness, and will continue to do so for the foreseeable future.
All of my research into the topic of longevity, continued to demonstrate this.
There are many different ‘types’ of exercise out there, many wide-reaching definitions and specific examples. But two aspects of it emerged as particularly important for longevity and healthspan during my research on the topic:
1) Resistance exercise (strength training) to build and maintain lean muscle mass; this fights ‘sarcopenia’, which is the loss of muscle mass with age
and
2) Aerobic (i.e. ‘Cardio’) exercise (i.e. training for your cardiovascular system), to strengthen the heart, lungs and circulatory system; this is unequivocally shown to prevent/delay the onset of cardiovascular disease, as well as activate a wide spectrum of protective benefits
Starting a regular exercise habit for longevity’s sake!
There are certainly many details that I could share from the past 18 months of my creating a new and enduring habit of regular cardio exercise, and I do hope to share that with you in the future. But I’d like to jump straight to the finish line, literally. Here is a post on my Instagram from last week, after winning a 5k race in Sydney:
I ran that 5K in 20:58! If I had even tried to run 5K back in May 2018, I wouldn’t have been able to complete the race.
So, how did I manage that? What did I do to get in shape?
I’m going to say that’s out of scope for this post, and may decide to share that information with you in the future. That’s not really the point here.
Your healthspan is YOUR responsibility
What is the point is this - one of the major themes of this blog is the power of proactive healthcare.
I’ve provided a bit of a definition on this concept in my opening post, but we’ll need to keep discussing the concept to make it clear what we mean by that term.
Let’s continue that process of elaboration! Proactive healthcare has two major components.
The first and most important part of proactive healthcare is intentionally owning the responsibility we have to our health. Simply put - it is your responsibility to stay healthy.
“The first and most important part of ‘proactive healthcare’ is intentionally owning the responsibility we have to our health. It is our (YOUR) responsibility to stay healthy”
This is an important difference from what has been engendered in our society - that this responsibility is that of your doctor.
Play that game if you want, but it will not necessarily lead you to the long and healthy life you deserve.
Don’t get me wrong - your doctor may be a fundamental part of the journey, but it starts with YOU.
So let me also ‘walk the talk’, as Dr. Sanders does. One of the key outcomes of my visit to the Health Nucleus was this realisation.
That living a long, healthy and happy life is MY responsibility - no one is going to do it for me!
And exercise (Strength and aerobic training) is inseparable from any longevity strategy. We’ll write more on this topic in the future.
Exercise comes first, sexy longevity technologies second
It’s only after we’ve begun to take the first part of the proactive healthcare concept seriously, that the second aspect truly becomes powerful.
This second aspect of proactive healthcare is demanding access to the best longevity technologies available.
If you want to be healthy and stay that way for as long as possible, visiting a preventative healthcare facility like the Health Nucleus is a great part of the overall strategy.
But if you decide to join me in this journey of biohacking our way through a long and healthy life, you will not escape making lifestyle changes.
How do I know? Because I had to drag my ‘cardio hating’ lazy ass out of bed and whip my butt into shape like my longevity depends on it! Because it does.
I took ownerships and established a ‘cardio’ routine
”That’s absolutely wonderful!” Dr. Sanders said, beaming. “I am just so impressed you were able to make that positive change so quickly and with such determination!”, she remarked.

5K races are my new jam
Staying motivated, staying healthy, staying young!
I’d just dropped the info that I’d actually taken my doctors advice.
We were on a ‘comprehensive return of results’ web video call, after our first ‘preliminary return of results call about 6 weeks earlier.
After the preliminary results call, my Health Nucleus blood results indicated that I was likely a good candidate for improving my results through - you guessed it, cardio exercise.
So, in the spirit of intentionally taking ownership of my health, I said to Dr. Sanders at the end of that first call, “Hey, I’m going to ask you to do something for me.”
“Sure” she volunteered willingly, “What might that be?”
“Please check in on how much cardio exercise I did between now and then!” I asked.
Well, she’d agreed, so I knew my ass was on the line!
That’s just one of the ‘mental hacks’ I used to get myself there. But it is a powerful one.
Is there someone in your life who can provide you with that accountability? If you know you need to ‘get fitter’, then I suggest you start that conversation.

Editorial Note: We have purposefully changed the name of the Health Nucleus Doctor in this story :)
What is a biohacker anyway? A simple definition
What is biohacking? Do I even biohack bro?

A selection of my supplement routine circa July 2019
A post by our Founder Dr Nick!
I’ve been loosely referring to myself as a ‘biohacker’ for a little over a year now. It’s a term that I’d adapted from my own interests in human longevity, and what I believe is an upcoming step-change in how long human beings will be able to lead healthy lives.
But it wasn’t until I came across this YouTube video that featured a discussion between the two authors of The Biohacker’s Handbook (read more), Dr. Olli Sovijärvi and Teemu Arina, where at ~28:45 into the interview video, they discussed the definition of ‘biohacking’
Biohacking = Preventative health
“I would use biohacking almost as a synonym for preventative healthcare” says Dr. Sovijärvi “At some point, ‘biohacking’ as a term might not be as relevant… the preventative healthcare system is just rising”
This really got me much more interested in the concept of being a biohacker and really broadened the definition of this term into an area that I really cared about.
My initial impressions of the term ‘biohacking’ used to draw out cognitive constructs of… let’s call them the more ‘creative’ types of humans who implant electronics or RFID chips beneath their skin or modify their genome by injecting themselves with CRISPR.
I’m not passing any judgment on those folks whatsoever - but I’m interested in a wider appeal with my sphere of influence. Something that my father or neighbour or peer can find interesting and accessible.
This conversation between two of the earlier members of the biohacking movement (who are now in their 5th year of organising the Biohacker Summit) and authors on one of the most popular books on the topic, offers us that broader, more widely relevant definition.
Perhaps we can even look to their book’s website, where ‘biohacking’ is even further defined in their landing page text:
Biohacker’s Handbook weaves together novel perspectives on technology, nature and self-development.A biohacker sees his or her body as a complex system that can be probed, analyzed, understood, and put under the test.
Such controlled experimentation (i.e. biohacking) can be used to pursue self-development and deeper self-understanding
Now we’ve expanded the territory even further.
A biohacker respects the complexity of biology, particularly that manifested in the human being, where our metaphysical elements of the mind & self-awareness are arguably as equally powerful as the physical systems that drive the body.
And respects that given this complexity, that experimentation, including the collection of data, outcomes, forming of hypotheses, is fundamental to the processes of biohacking.
And let’s not skip over the last part - that all of these actions are in pursuit of deeper self-understanding and self-development.
I like to think of this process within myself as a continual optimisation of my overall ‘well-being’ (more on that in the future).
Are you a biohacker?
I routinely collect biometric data (blood glucose, blood pressure, blood ketones, heart-rate).
I run experiments upon myself in the pursuit of deeper self-understanding (eating a ketogenic diet for a year in 2018, fasting for 3-5x days per month in 2019).
I also engage with technologies that are best classified as ‘preventative healthcare’ - look no further than my visit to the Health Nucleus in May 2018.
Each day, I take approximately 30 supplements, collect increasing amounts of biometric data, and routinely partake in high-intensity interval and strength exercise to stimulate my mitochondria and up-regulate my glucose metabolism…. and that’s just the start!
So, would I call myself a biohacker?
Definitely worth your cash, if you’re into health optimisation. Snag a copy? It’s a great place to start your biohacking journey.
Hell yes I would.
But what I would like to see, more than anything, is more folks joining the biohacker movement.
This is a broader category of health conscious humans, who are using novel methods of measuring their overall health (like biological age), to run self-experiments.
One of the main reason I founded Longevity Blog is to help you learn how to collect your blood, try longevity interventions and be able to determine if they work for you.
We just might make a biohacker out of you yet!






3 Technologies for Monitoring Heart Health
Three heart health technologies looking after your ticker
Monitoring heart health is a top priority. When it comes to listing your vital organs - those needed most for your overall well-being and the joy of being alive, the heart comes up at the top of the list (along with your brain, liver, kidneys…).
It should be at the top of the list for all longevity enthusiasts keen to look after their long-term health. But what technologies are accessible and valuable for this purpose?
Heart Health and the EKG
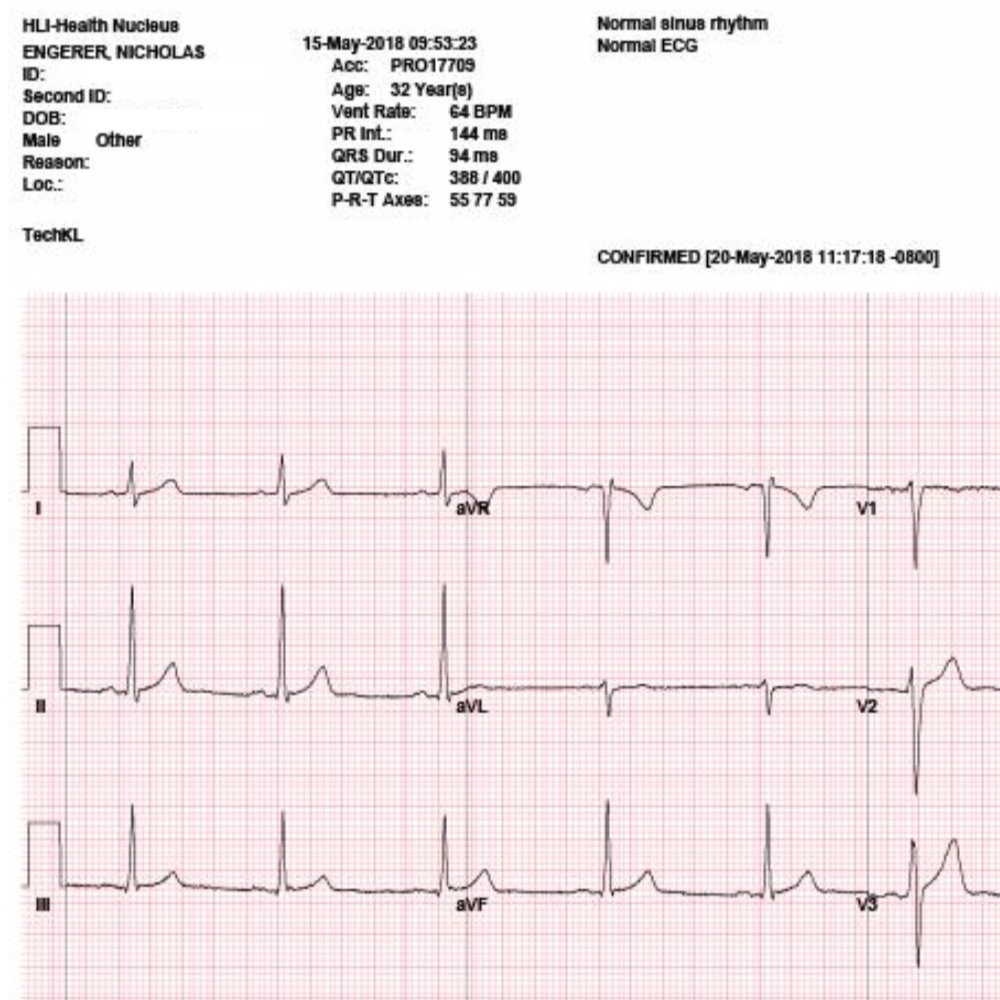
Health Nucleus EKG results for Nick were all fine and dandy!
An EKG is short for ‘electrocardiogram’. The EKG is on the frontlines for assessing heart health, and is particularly valuable in the case of an ongoing heart attack.
An EKG is completed by checking the electrical activity of the heart by attaching several small sticky electrode pads to your arms, chest and legs.
The EKG provides the following information:
Analysis of blood flow to your heart muscle
The electrical signals of heart rhythm
A first line of detection for abnormalities
Detect electrolyte imbalances
What’s fascinating about EKGs is how accessible the technology has recently become.
Perhaps the biggest impact on accessibility of this test has been made possible by the Apple Watch, for which Series 4 and above have EKG capabilities
But the Apple Watch is not alone! Several other ‘test at home’ technologies are also available. “Emay” is another technology brand which has entered the space.
They have an impressively compact and slick device, which we personally prefer over the Apple Watch due to its lower cost and dedicated function (does an iMessage on your wrist help your heart health?).
Don’t get confused about the “ECG” term, EKGs and ECGs are the same test.
Heart Health and Cardiac MRI
In an earlier post we discussed the merits of full body MRI and cardiac MRI.

Example of Nick’s cardiac MRI findings. Note the very particular measurements of the heart anatomy.
MRI stands for magnetic resonance imaging. A heart or cardiac MRI looks into the structures of the heart and its neighbouring blood vessels in great detail.
A Heart/Cardiac MRI is used to diagnose/check for:
early signs of heart disease
assess the the heart for any signs of damage
detect any imminent heart failure or defects
assess inflammation of the membrane lining the heart
While you certainly can’t perform a cardiac MRI at home, you can work with organisations like the Health Nucleus or a specialist to have these tests completed.
Heart Health and THE ZIO

Wearing the Zio
Two weeks of detailed heart-rate data, under all conditions - exercise, rest, day-to-day activity. Including tracked events where Nick pushed the button for closer inspection in the report (see below).
As a part of Nick’s preliminary Health Nucleus visit, he was sent away with a small stick-on device called a ‘Zio’ that he wore for two weeks.
The Zio watches heart-rate in great detail and and includes the ability for the user to track events of interest by clicking the device.
Nick noted he ‘clicked’ the button on a few events where his heart-rate seemed to pick-up and beat hard after lying down in my bed.
He’d actually noticed these events for most of his adult life, and had passing concern about what that indicated about my heart/body health.
Those events have now been analysed in great detail and revealed no underlying heart driven worries.
The Zio device is attached with a gentle adhesive which did not cause any skin irritation.
Beyond having to ‘bag’ the device in order to take a shower (covering it with plastic and tape), it is a very easy device to manage.

Notes from Nick: “Those ‘Black dots’ are regions where I clicked the button for closer inspection. These were events where I noticed my heart-rate seeming to pick-up, or be more noticeable after lying down in my bed.
I’d noticed these my whole life - now I know they have no underlying heart driven worries and can rest easy :)”

Zio IRhythm overall report after two weeks
Nick’s Zio report. 175bpm during an intense workout. 52 bpm minimum recorded during the overnight.
FDA & TGA DISCLAIMER
This information is intended for educational purposes only and is not meant to substitute for medical care or to prescribe treatment for any specific health condition. These blog posts are not intended to diagnose, treat, cure or prevent any disease, and only may become actionable through consultation with a medical professional.

Full body MRI data: health screening of the brain, heart and abdomen
What is a 3D full body MRI and what did I learn from completing one at the Health Nucleus in San Diego?
Full body MRI scan technology
Full body MRI data is an incredible advancement for health screening.
As we covered in our inaugrual post, our Founder (Nick), chose the Human Longevity Inc ‘Health Nucleus’ in 2018 as the starting point for his personal comprehensive health screening journey.
The San Diego based centre, focuses on employing cutting edge capabilities for detecting disease at an early stage. Full body MRI scanning is core to their offering.
This post offers a quick overview at what this technology is capable of.
What is a full body MRI? (With Video)
Magnetic resonance imaging (MRI) has the ability to image the inside of your body in great detail, through the use of strong magnetic fields and radio waves. It does this without the use of harmful electromagnetic radiation (like X-rays or CT scans).
At the Health Nucleus, the full body MRI scan emphasises the brain, cardiac health and cancer screening within the chest, abdomen and pelvis. It also produces valuable information about body composition.
Here is a great short video from HLI that you can view below that explains this a bit further:

Why purchase a Full body MRI?
The future of healthcare is proactive & preventative, and that future is underpinned by comprehensive health screening technologies like the full body MRI!
The current state of ‘reactive healthcare’ (only treat you once you are sick), has already pioneered nearly all of the medical treatments required to treat the most common life-threatening diseases.
This however requires that they are detected early at the ‘treatable stage’. This is where full body MRI scanning comes in handy.
A full body MRI like the one offered by the Health Nucleus, scans the brain, heart and abdomen in high resolution. Through their specialised suite of sophisticated post-processing algorithms, they are able to detect tumours that are only millimetres in diameter.
This technology can also discover brain aneurisms before they ruptures, as well as abnormalities of the heart or circulatory system.
You may be surprised to know that the Health Nucleus has found clinically significant findings in 40% of their clients! These aren’t all revealed by the full body MRI, but many of the more serious and dangerous findings are (e.g. pancreatic cancer).
What is a full body MRI experience like?
A fully body MRIO requires being inside of an MRI machine for up to 70 minutes (with a short break in between). This can be quite intimidating for some people.
Here is a short video describing Nick’s full body MRI experience:
What did a FULL body MRI reveal about me?

““I spent nearly 75 minutes in the MRI machine, watching amazing images from outer space on a ceiling-mounted monitor, while listening to relaxing transcendental music””
Example full body MRI data - The Brain

Brain analytics, highlighting the different regions of Nick’s brain.
As is the case for many folks undertaking proactive health screenings, Nick’s full body MRI did not reveal any pathological findings.
What was gathered however, was a wealth of valuable baseline data. As an example, the brain scanning established normal values for the volumes of each of the major regions of the brain.
One area of particular interest is the hippocampus, whose volume is known to decrease with age, along with a decline in short-term memory and overall ‘plasticity’ (ability to adapt to new learning).
As Nick ages, we’ll be able to monitor his hippocampus for any changes in its volume. As well as other regions under increased pressure with aging, such as the hypothalamus.
Example of full body MRI data - The Heart

Nick’s heart beating away!
Cardiac MRI is a specific type of scanning approach, which can watch the heart beat and trace the flow of blood.
For example, the ‘ejection fraction’ can be quantified, and tracked over time. Any abnormalities in heartbeat are also immediately apparent.
Cardiac MRI reveals the structure of the heart, and in particularly can detect any hypertrophy (abnormal growth of a heart chamber) or thickening of the heart wall because of high blood pressure.
Example of fully body MRI data - Visceral fat

MRI data is also exceptional at revealing body composition.
One of the more important predictors of the risk of disease and/or mortality (risk of dying) are an individual’s visceral fat levels.
Another important metric is the total volume of fat in your liver (e.g. fatty liver disease).
The full-body MRI can directly quantify these volumes, compare you to a reference population and give you clear advice on how much fat you need to lose to lower your disease risk.



FDA & TGA DISCLAIMER
This information is intended for educational purposes only and is not meant to substitute for medical care or to prescribe treatment for any specific health condition. These blog posts are not intended to diagnose, treat, cure or prevent any disease, and only may become actionable through consultation with a medical professional.

Comprehensive health screening: Health Nucleus
Health screening is the future of healthcare

In this short 5-minute video, our founder shares personal thoughts on the future of healthcare, and why it is proactive. The technologies to prevent disease are at your disposal, will you choose to access them?
Medical screening in great socks

The future of healthcare
includes great socks 🧦
The future of healthcare is based on health screening that is proactive & preventative!
Today, we have all of the medical technology required to detect and treat the most common life-threatening diseases, provided that we can detect them early on.
This includes common killers such as cardiovascular disease (heart-attack, stroke, thrombosis), the chronic illnesses of metabolic disease (diabetes) and, of course, most cancers.
Even health screening and early detection of diseases of the brain (alzheimer's or parkinson’s) can result in extended healthspan, and slow the rate of disease progression (although a cure for these maladies will likely require changing the ageing process itself!)
Health screening gets personal
As our founder shares, health screening is part of a personal motivation for creating Longevity Blog. “In my late 20s, I had three people quite close to me, also in their late 20s, be diagnosed with cancer. In fact, one of them, was my own wife (appendix cancer)!”
“Another had stage III colon cancer. The third, stage IV testicular cancer that nearly took his life.”
In each of these cases, treatments came well after the onset of the disease, which brought on deeper thoughts on the very nature of how we detect and treat these diseases.
Health screening is how healthcare catches up to the 21st century
New longevity technologies are being developed and deployed at an increasing pace. Some forward thinkers, including our Founder, observe this trend to be exponential in nature.
This is particularly true for health screening technologies which are directly coupled with progress in computing capabilities (processing power, network communication speeds, memory availability).
However, your personal experience in the healthcare system does not make these changes immediately evident. The healthcare system has made great strides in responsive medicine - treating disease at later stages, after an acute event or advance systems are present.
Comprehensive regular health screening is available now
All of the health screening technologies required to detect diseases at an early, highly treatable stage exist NOW (at the time of writing, late 2019).
It is not technological limitations which prevents your access to these technologies. Instead, the limitations are based on 1) knowledge of alternatives, 2) financial means to access them, and 3) your personal demand for access to them.
This foundational post from the Longevity Blog will be followed by all of the information you’ll require to learn about proactive healthcare technologies and how to access them.
It will include our Founder’s personal foray into this technology space, where we’ll use his experience to thoroughly vet and explore these new technologies, to help you decide which to add to your own personalised longevity strategy.
FULL BODY HEALTH SCREENING: the Health Nucleus
Full Body 3D MRI - on the cutting edge of proactive healthcare
As you’ll soon learn, many forward thinking technologists, scientists and medical professionals have already begun to create a healthcare system worthy of the 21st Century.
Where this adventure will start, is at one of the most comprehensive health screening treatment centres in the world: Human Longevity Inc’s Health Nucleus.
Based in San Diego, California, our Founder first visited the Health Nucleus in May 2018. Where he underwent the following:
a wide-reaching blood panel
microbiome sequencing (💩)
What followed on from this visit was a complete transformation in his approach to health and wellness. It’s precisely this type of self-experimenting that helps us create unique content to guide you on your own wellness journey.
Read more about the Health Nucleus in the following posts:









